

Prevalence and healthcare burden of pulmonary alveolar proteinosis
- PMID: 30064481
- PMCID: PMC6069872
- DOI: 10.1186/s13023-018-0846-y
Prevalence and healthcare burden of pulmonary alveolar proteinosis
Abstract
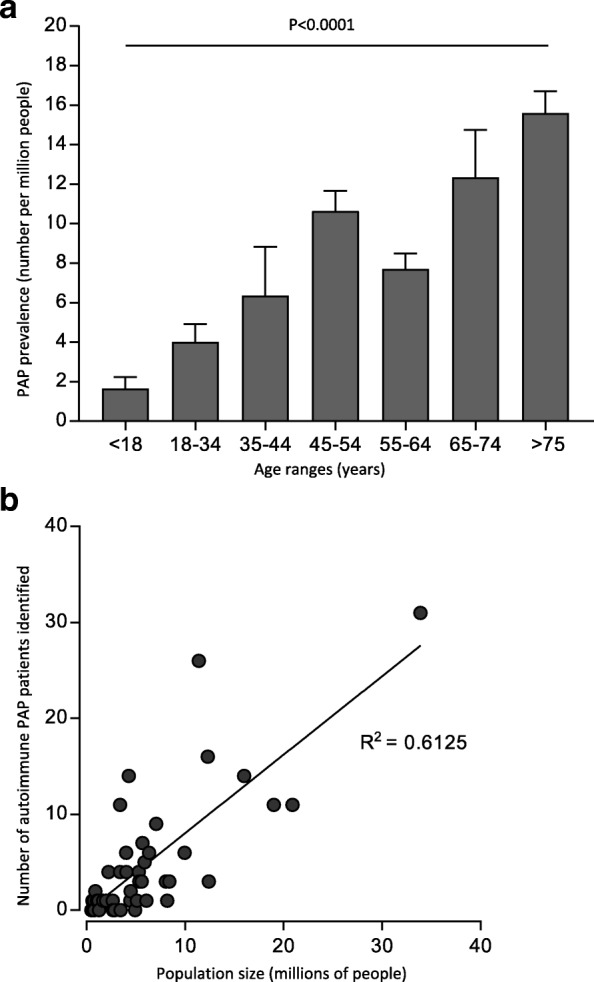
Pulmonary alveolar proteinosis (PAP) is a rare syndrome of alveolar surfactant accumulation, resulting hypoxemic respiratory failure, and increased infection risk. Despite advances in our understanding of disease pathogenesis and the availability of improved diagnostics, the epidemiology and healthcare burden of PAP remain poorly defined. To determine the prevalence, and healthcare utilization and costs associated with PAP, we interrogated a large health insurance claims database containing comprehensive data for approximately 15 million patients in the United States. We also evaluated data from a referral-based diagnostic testing program collected over a 15-year period. The prevalence of PAP was determined to be 6.87 ± 0.33 per million in the general population, similar in males and females, and increased with age, however considering difficulties and delays in diagnosing this is likely a minimum estimate of true prevalence. PAP patients had significantly more comorbidities, health care utilization and associated costs compared to control patients precisely matched for age and gender. Between 2004 and 2018, 249 patients confirmed to have PAP were evaluated to identify the PAP-causing disease; 91.5% had autoimmune PAP, 3% had hereditary PAP caused by GM-CSF receptor mutations, 4% had secondary PAP, and 1.5% had congenital PAP. Considering the high diagnostic accuracy of serum GM-CSF autoantibody testing and predominance of autoimmune PAP, these results emphasize the importance of utilizing blood-based testing in PAP syndrome to identify the PAP-causing disease rather than invasive lung biopsies, resulting in earlier diagnosis, reduced morbidity and lower healthcare costs.
Keywords: GM-CSF autoantibody; Healthcare burden; Prevalence; Pulmonary alveolar proteinosis.
Conflict of interest statement
Ethics approval and consent to participate
The institutional review board of Cincinnati Children’s Hospital Medical Center a approved the study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Sakagami T, Beck D, Uchida K, Suzuki T, Carey BC, Nakata K, Keller G, Wood RE, Wert SE, Ikegami M, Whitsett JA, Luisetti M, Davies S, Krischer JP, Brody A, Ryckman F, Trapnell BC. Patient-derived granulocyte/macrophage colony-stimulating factor autoantibodies reproduce pulmonary alveolar proteinosis in nonhuman primates. Am J Respir Crit Care Med. 2010;182:49–61. doi: 10.1164/rccm.201001-0008OC. - DOI - PMC - PubMed
-
- Suzuki T, Sakagami T, Young LR, Carey BC, Wood RE, Luisetti M, Wert SE, Rubin BK, Kevill K, Chalk C, Whitsett JA, Stevens C, Nogee LM, Campo I, Trapnell BC. Hereditary pulmonary alveolar proteinosis: pathogenesis, presentation, diagnosis, and therapy. Am J Respir Crit Care Med. 2010;182:1292–1304. doi: 10.1164/rccm.201002-0271OC. - DOI - PMC - PubMed
-
- Available from: https://www.optum.com.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
