

High prevalence of epilepsy in onchocerciasis endemic health areas in Democratic Republic of the Congo
- PMID: 30064504
- PMCID: PMC6069757
- DOI: 10.1186/s40249-018-0452-1
High prevalence of epilepsy in onchocerciasis endemic health areas in Democratic Republic of the Congo
Abstract
Background: A high prevalence of epilepsy has been observed in many onchocerciasis endemic regions. This study is to estimate the prevalence of active epilepsy and exposure to Onchocerca volvulus infection in a rural population in Ituri province, Democratic Republic of Congo.
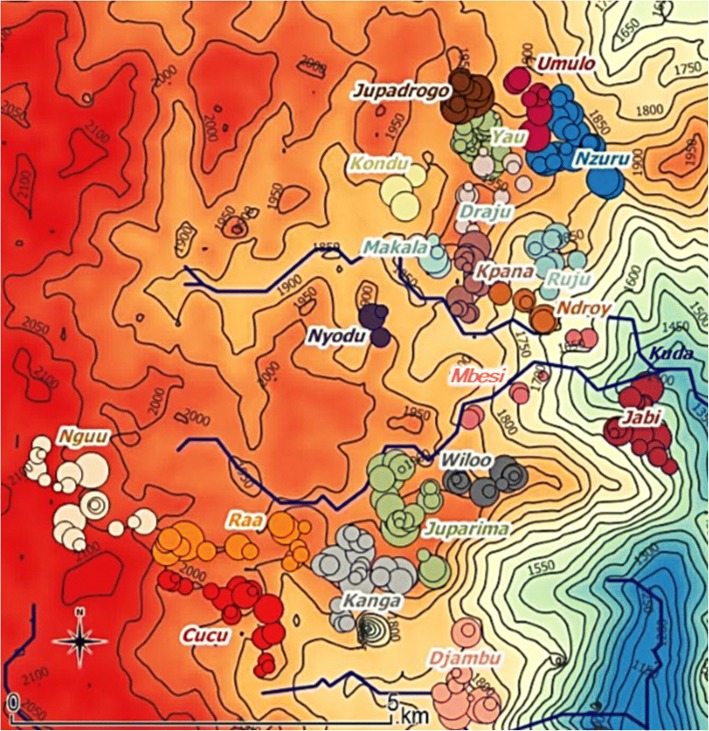
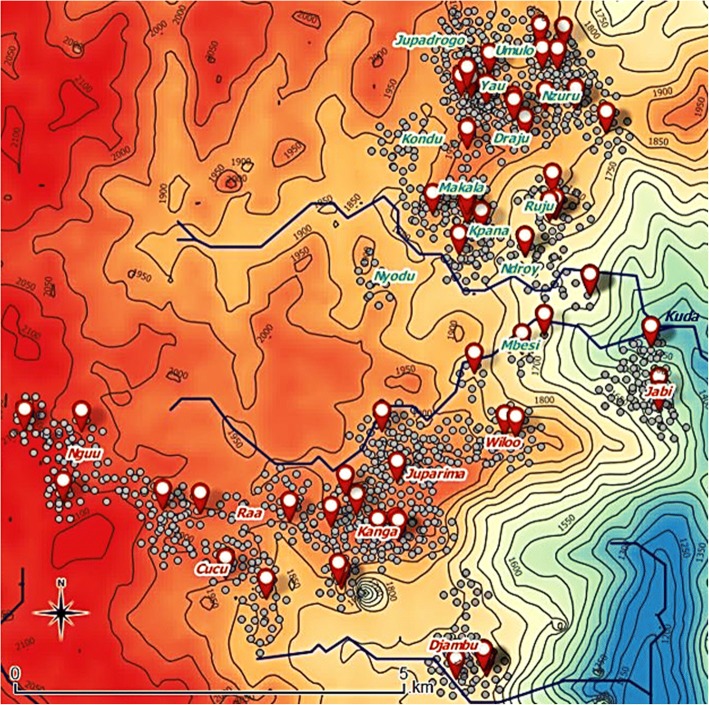
Methods: In August 2016, a community-based cross-sectional study was conducted in an onchocerciasis endemic area in the rural health zone of Logo, Ituri Province. Households within two neighbouring health areas were randomly sampled. To identify persons with epilepsy, a three-stage approach was used. In the first stage, all individuals of the selected households were screened for epilepsy by non-medical field workers using a validated 5-item questionnaire. In the second and third stage, suspected cases of epilepsy were examined by non-specialist medical doctors, and by a neurologist, respectively. A case of epilepsy was defined according to the 2014 International League Against Epilepsy (ILAE) guidelines. Exposure to O. volvulus was assessed by testing for IgG4 antibodies to an O. volvulus antigen (OV16 Rapid Test,) in individuals aged 3 years and older.
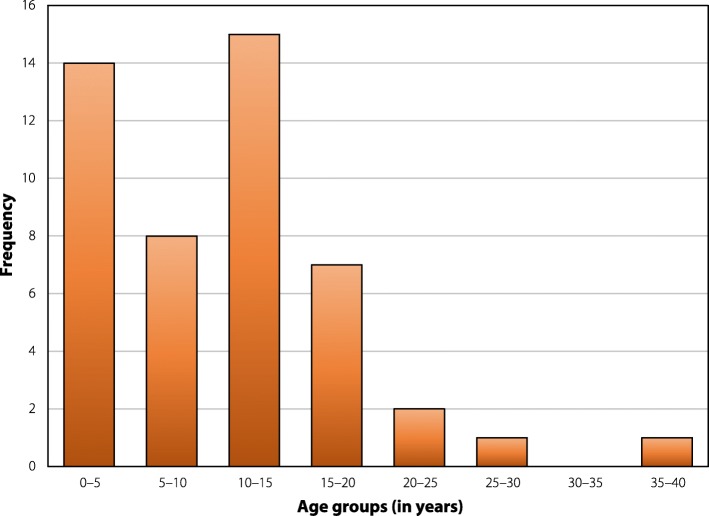
Results: Out of 1389 participants included in the survey, 64 were considered to have active epilepsy (prevalence 4.6%) (95% confidence interval [CI]: 3.6-5.8). The highest age-specific epilepsy prevalence estimate was observed in those aged 20 to 29 years (8.2%). Median age of epilepsy onset was 10 years, with a peak incidence of epilepsy in the 10 to 15 year-old age group. OV16 test results were available for 912 participants, of whom 30.5% (95% CI, 27.6-33.6) tested positive. The prevalence of OV16 positivity in a village ranged from 8.6 to 68.0%. After adjusting for age, gender and ivermectin use, a significant association between exposure to onchocerciasis and epilepsy was observed (adjusted odds ratio = 3.19, 95% CI: 1.63-5.64) (P < 0.001).
Conclusions: A high prevalence of epilepsy and a significant association between epilepsy and exposure to O. volvulus were observed in the population in Ituri province, Democratic Republic of Congo. There is an urgent need to implement a CDTI programme and to scale up an epilepsy treatment and care programme.
Keywords: Democratic Republic of Congo; Onchocerciasis; epilepsy; Prevalence.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Ethical Review Board of the University of Antwerp, Belgium and the Ethical Review Committee of Ngaliema Hospital, Kinshasa, DRC. Informed consent was obtained from the head of the village, the head of the household and from all adults belonging to the household. In case of children/minors/invalid adults, informed consent was obtained from the parents/caregivers. Those aged 12 years and older were asked to sign a supplementary section on the form stating their voluntary approval of participation. Participants were free to abstain from participation in the study or to withdraw consent to participate at any time. No direct benefits for participation in the study were provided.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Figures




References
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet 2017. 10.1016/S0140-6736(17)32154-2. - PMC - PubMed
-
- Makenga Bof JC, Maketa V, Bakajika DK, Ntumba F, Mpunga D, Murdoch ME, et al. Onchocerciasis control in the Democratic Republic of Congo (DRC): challenges in a post-war environment. Tropical Med Int Health. 2015. 10.1111/tmi.12397. - PubMed
-
- WHO . Onchocerciasis Fact Sheet. Geneva: World Health Organization; 2017.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
