

Encapsulating peritoneal sclerosis
- PMID: 30065556
- PMCID: PMC6064970
- DOI: 10.3748/wjg.v24.i28.3101
Encapsulating peritoneal sclerosis
Abstract
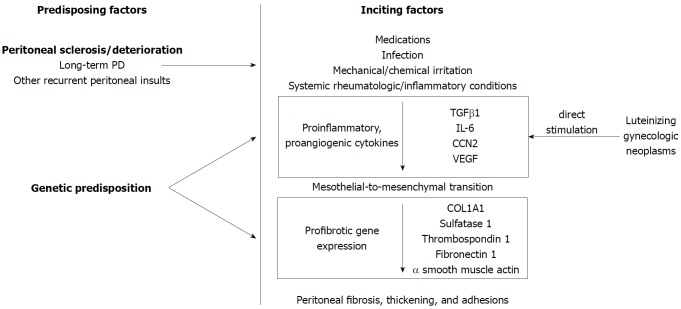
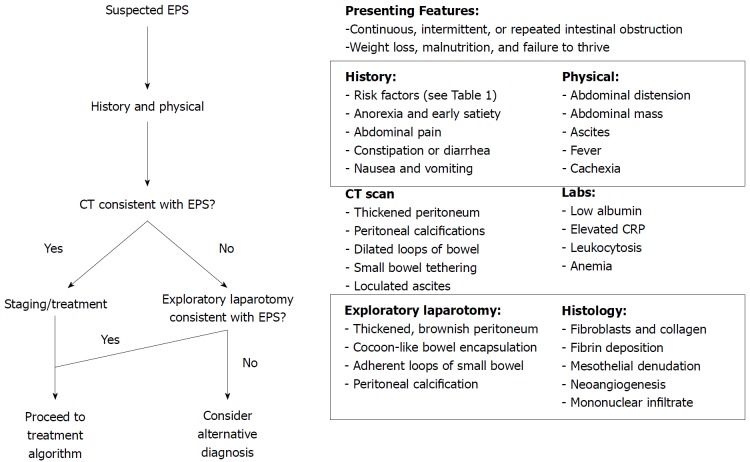
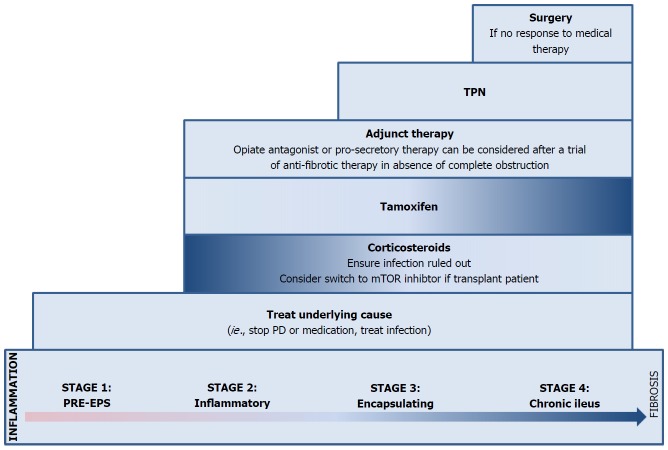
Encapsulating peritoneal sclerosis (EPS) is a debilitating condition characterized by a fibrocollagenous membrane encasing the small intestine, resulting in recurrent small bowel obstructions. EPS is most commonly associated with long-term peritoneal dialysis, though medications, peritoneal infection, and systemic inflammatory disorders have been implicated. Many cases remain idiopathic. Diagnosis is often delayed given the rarity of the disorder combined with non-specific symptoms and laboratory findings. Although cross-sectional imaging with computed tomography of the abdomen can be suggestive of the disorder, many patients undergo exploratory laparotomy for diagnosis. Mortality approaches 50% one year after diagnosis. Treatment for EPS involves treating the underlying condition or eliminating possible inciting agents (i.e. peritoneal dialysis, medications, infections) and nutritional support, frequently with total parenteral nutrition. EPS-specific treatment depends on the disease stage. In the inflammatory stage, corticosteroids are the treatment of choice, while in the fibrotic stage, tamoxifen may be beneficial. In practice, distinguishing between stages may be difficult and both may be used. Surgical intervention, consisting of peritonectomy and enterolysis, is time-consuming and high-risk and is reserved for situations in which conservative medical therapy fails in institutions with surgical expertise in this area. Herein we review the available literature of the etiology, pathogenesis, diagnosis, and treatment of this rare, but potentially devastating disease.
Keywords: Abdominal cocoon; Corticosteroids; Enterolysis; Peritoneal dialysis; Peritoneal sclerosis; Peritonectomy; Sclerosing encapsulating peritonitis; Tamoxifen.
Figures
References
-
- Kawaguchi Y, Kawanishi H, Mujais S, Topley N, Oreopoulos DG. Encapsulating peritoneal sclerosis: definition, etiology, diagnosis, and treatment. International Society for Peritoneal Dialysis Ad Hoc Committee on Ultrafiltration Management in Peritoneal Dialysis. Perit Dial Int. 2000;20 Suppl 4:S43–S55. - PubMed
-
- Owtschinnikow PJ. Peritonitis chronica fibrosa incapsulata. Arch für Klin Chir. 1907;83:623–634.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
