

An easier and safe affair, pleural drainage with ultrasound in critical patient: a technical note
- PMID: 30066098
- PMCID: PMC6068051
- DOI: 10.1186/s13089-018-0098-z
An easier and safe affair, pleural drainage with ultrasound in critical patient: a technical note
Abstract
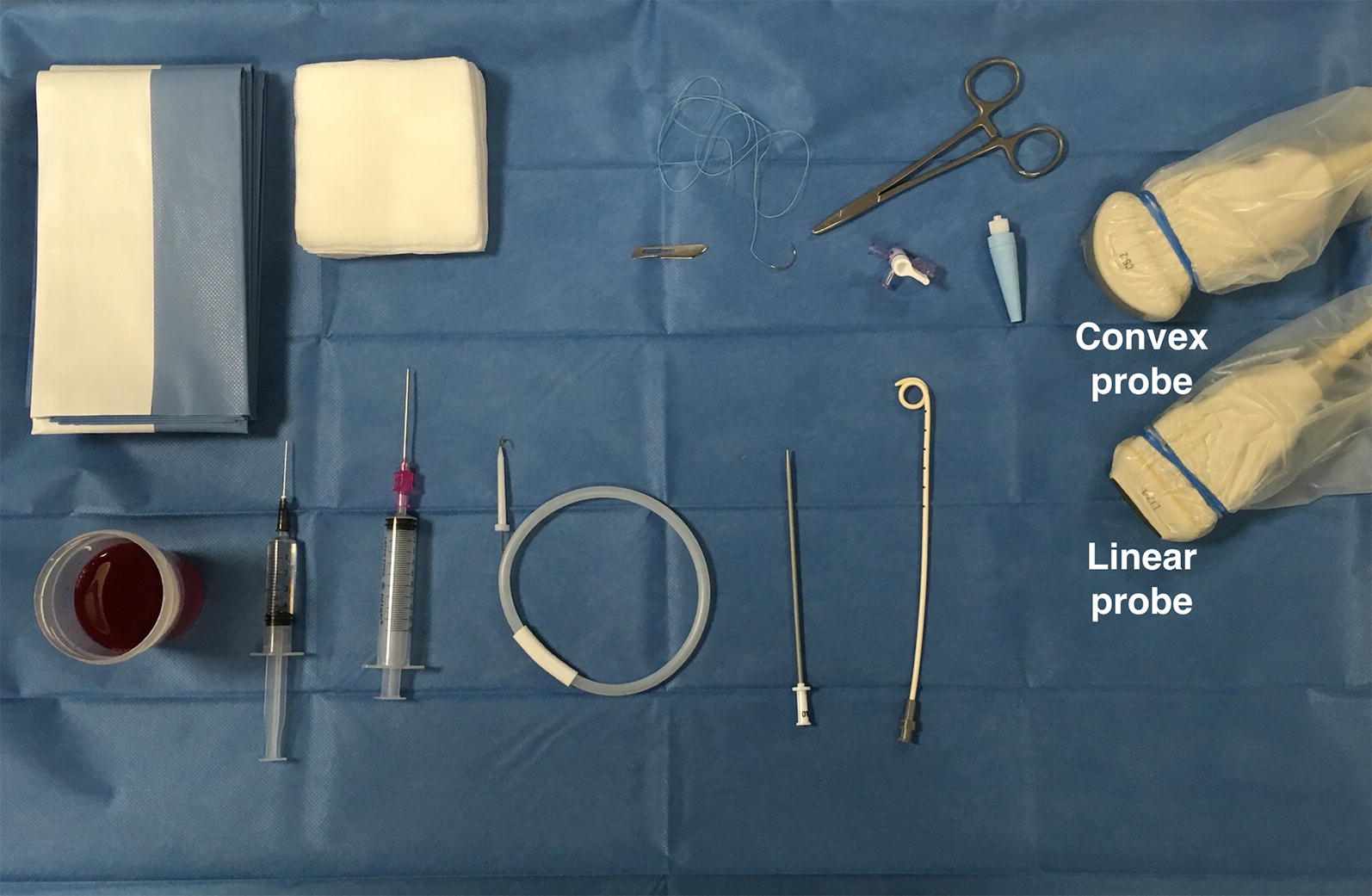
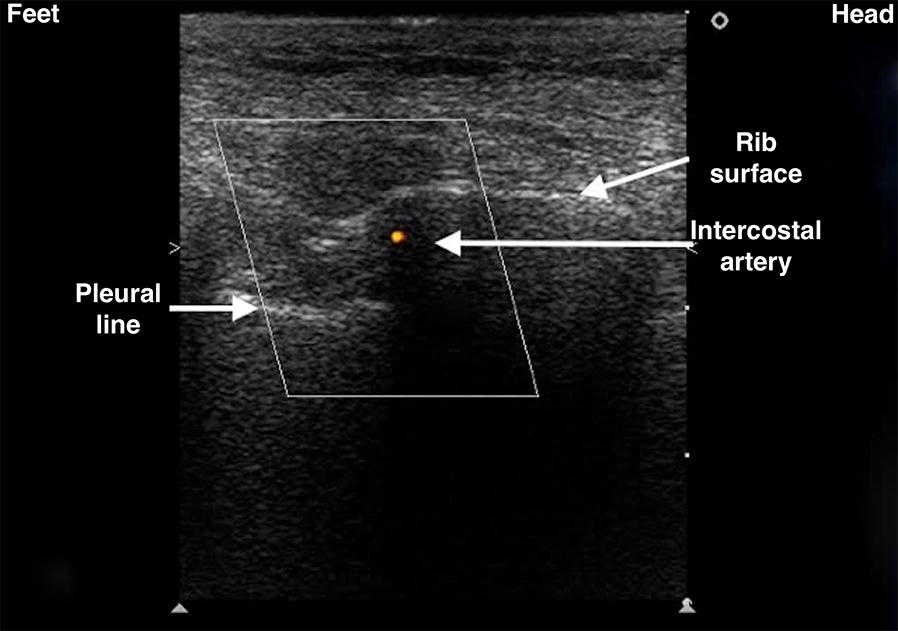
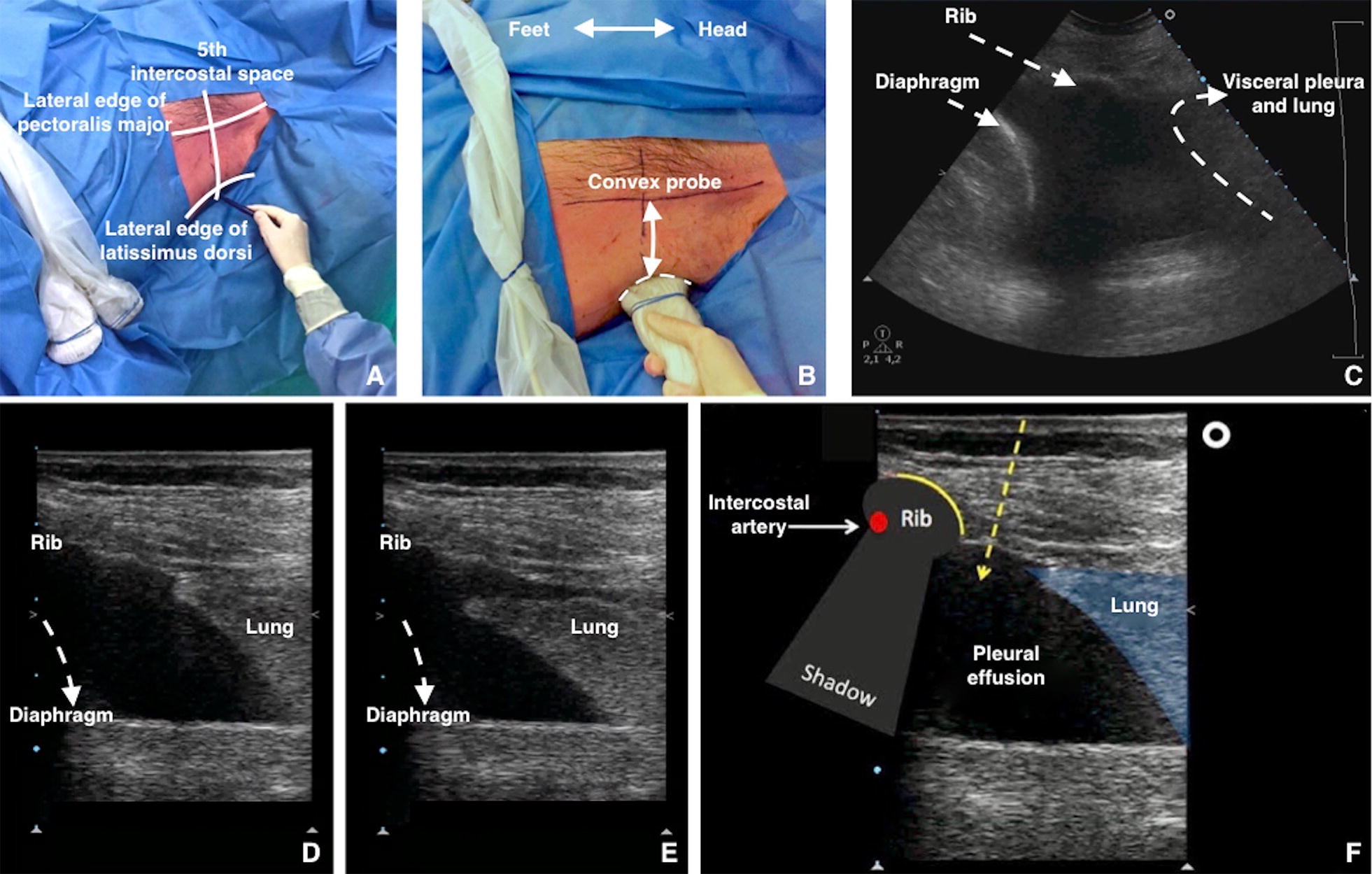
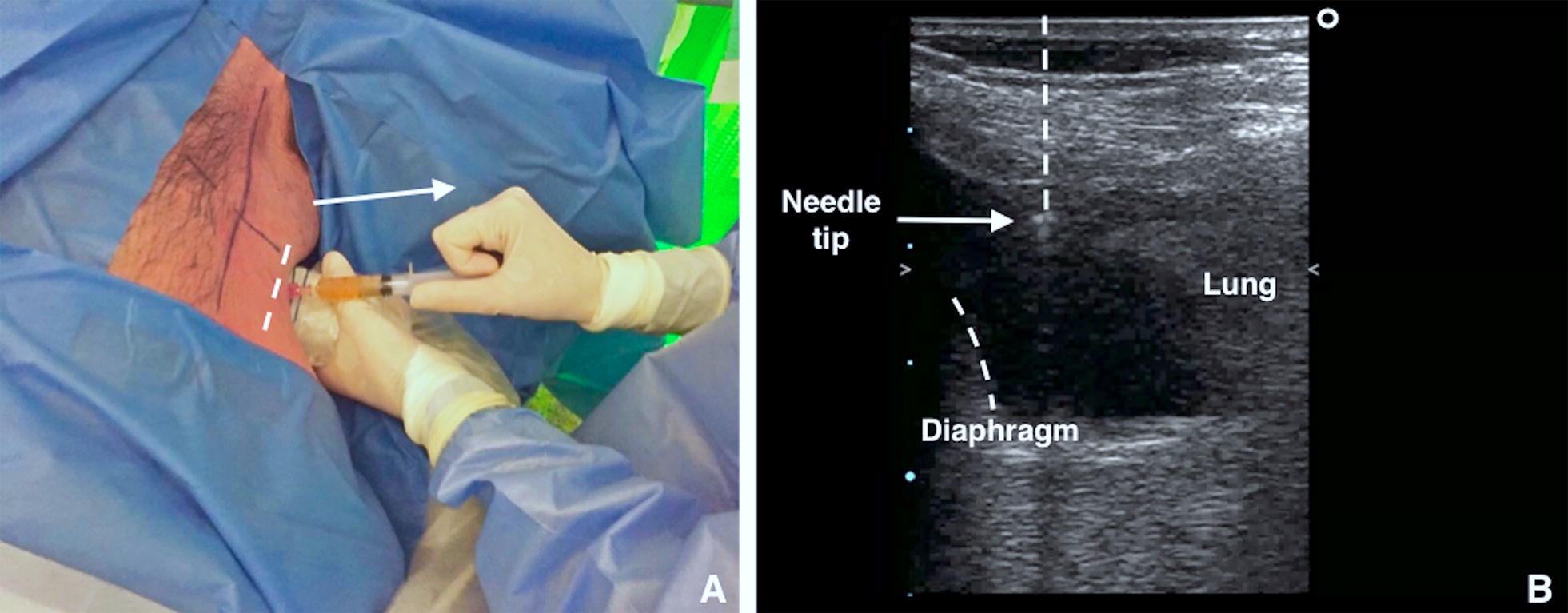
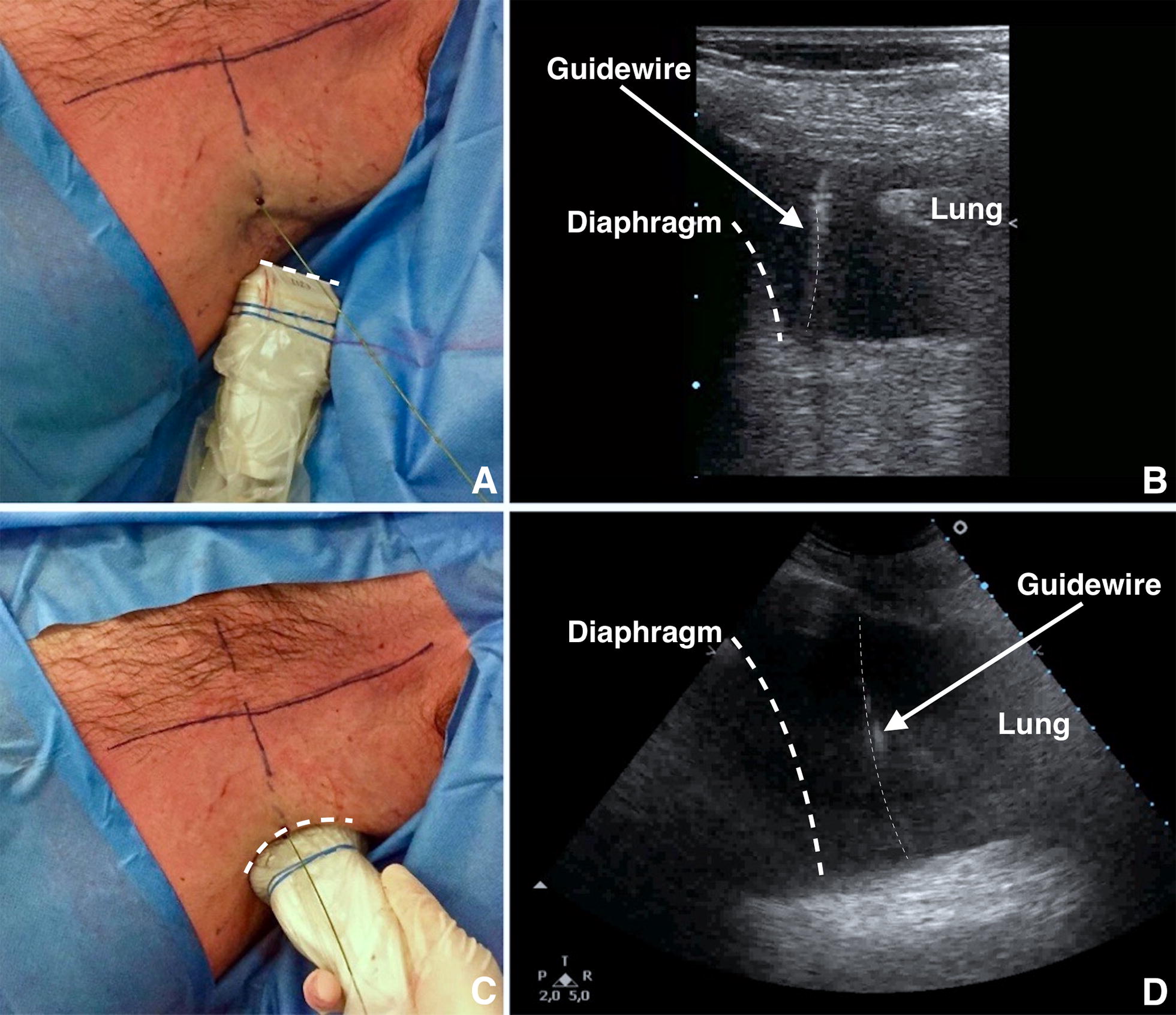
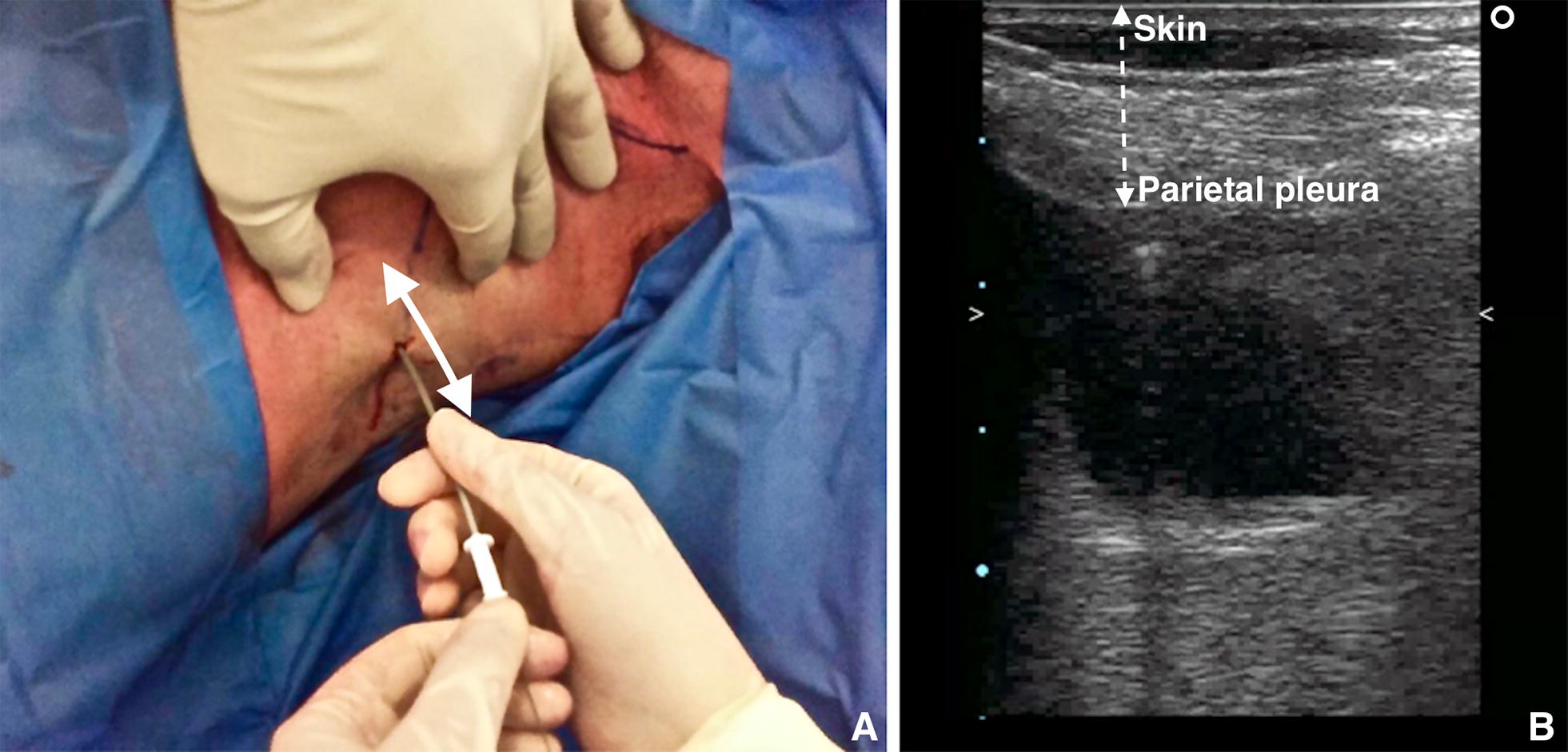
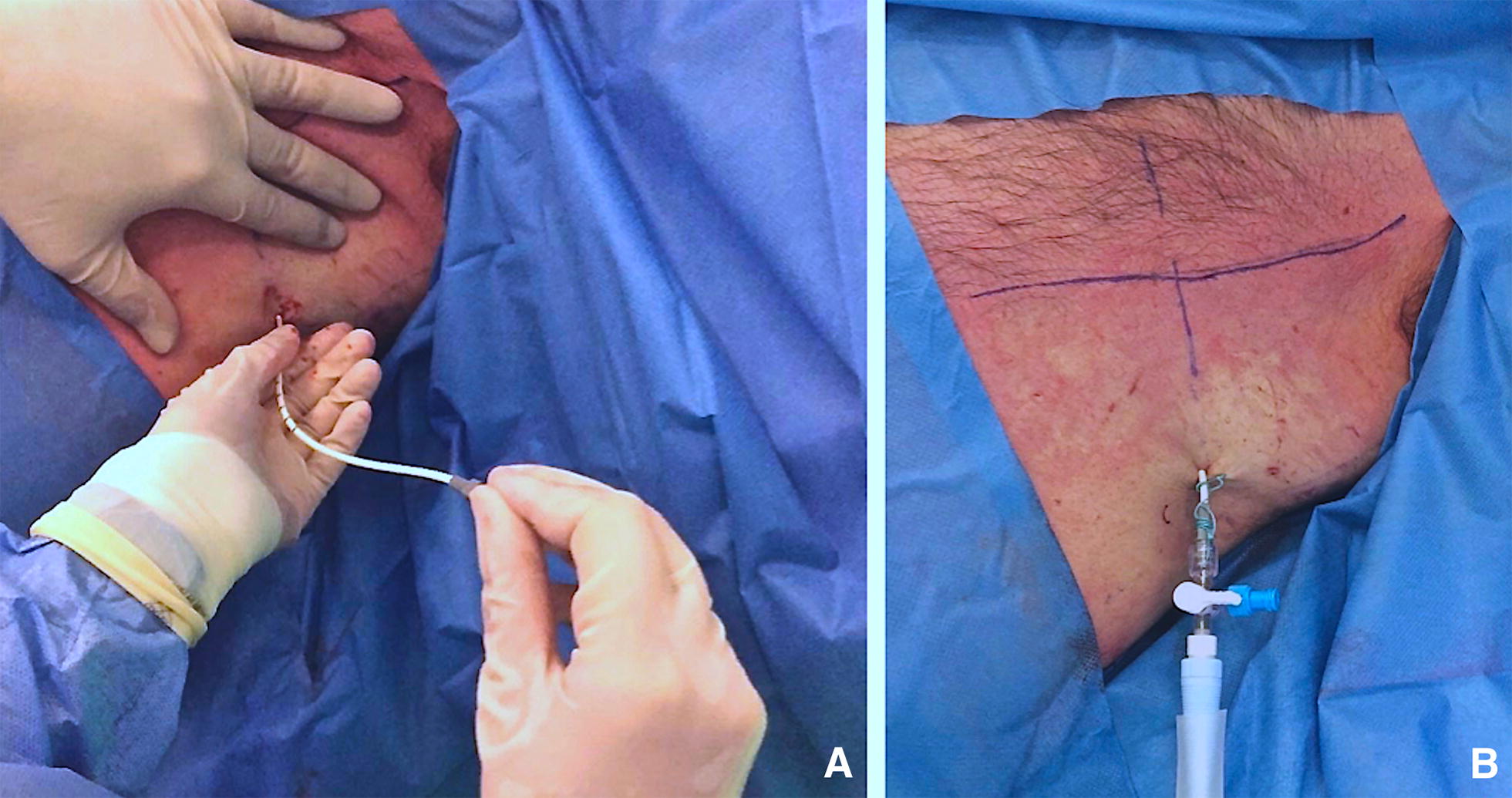
Thoracic ultrasound is a powerful diagnostic imaging technique for pleural space disorders. In addition to visualising pleural effusion, thoracic ultrasound also helps clinicians to identify the best puncture site and to guide the drainage insertion procedure. Thoracic ultrasound is essential during these invasive manoeuvres to increase safety and decrease potential life-threatening complications. This paper provides a technical description of pigtail-type drainage insertion using thoracic ultrasound, paying particular attention to indications, contraindications, ultrasound guidance, preparation/equipment, procedure and complications.
Keywords: Pleural drainage; Pleural effusion; Thoracic ultrasound; Ultrasound guidance.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
