

Comparative cost-effectiveness analysis of the subacromial spacer for irreparable and massive rotator cuff tears
- PMID: 30066101
- PMCID: PMC6399196
- DOI: 10.1007/s00264-018-4065-x
Comparative cost-effectiveness analysis of the subacromial spacer for irreparable and massive rotator cuff tears
Abstract
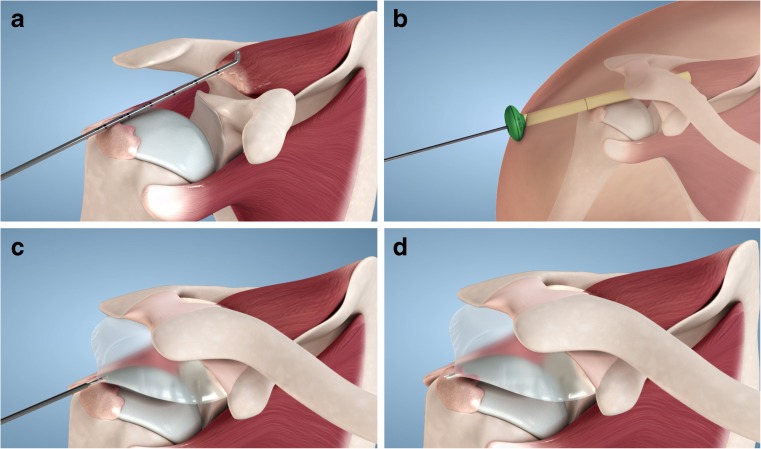
Purpose: There is ongoing debate regarding the optimal surgical treatment of irreparable rotator cuff tears (IRCT). This study aimed to assess within the Italian health care system the cost-effectiveness of subacromial spacer as a treatment modality for patients with IRCT.
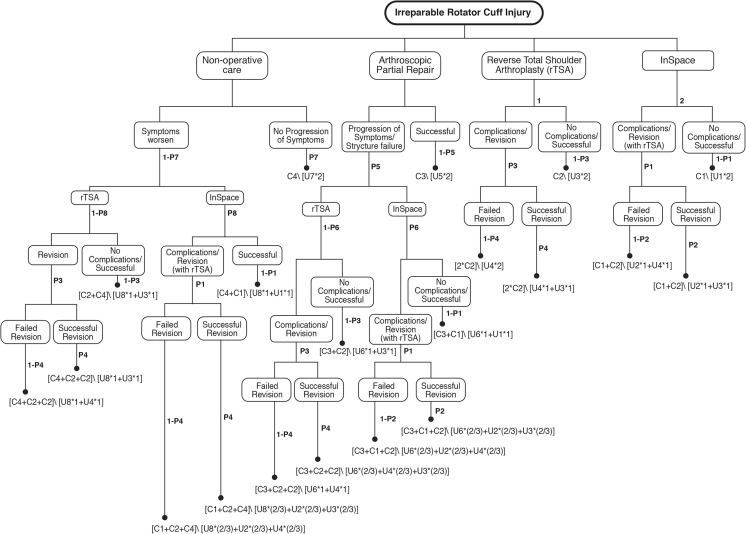
Methods: An expected-value decision analysis was created comparing costs and outcomes of patients undergoing arthroscopic subacromial spacer implantation, rotator cuff repair (RCR), total shoulder arthroplasty, and conservative treatment for IRCTs. A broad literature search provided input data to extrapolate and inform treatment success and failure rates, costs, and health utility states for these outcomes. The primary outcome assessed was an incremental cost-effectiveness ratio (ICER) of subacromial spacer implantation versus shoulder arthroplasty, RCR, and conservative treatment.
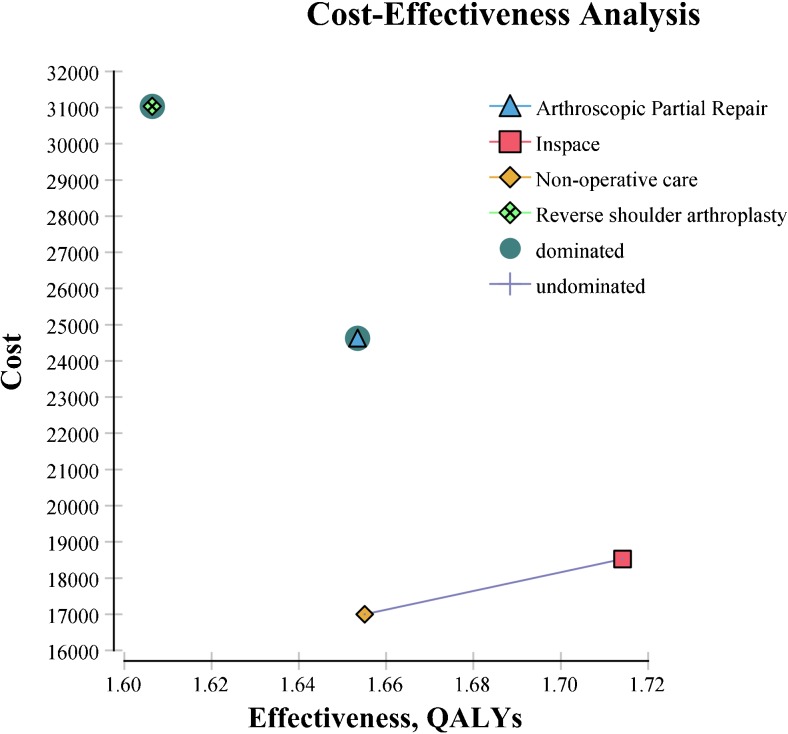
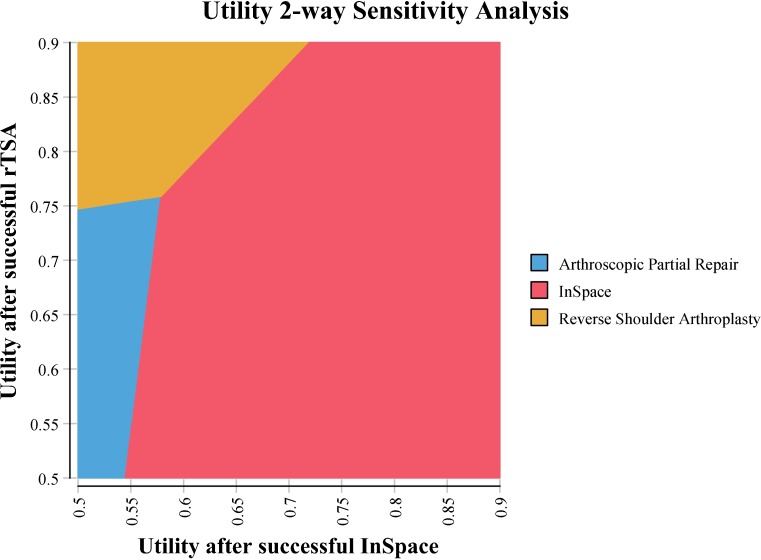
Results: Subacromial spacer is favorable over both arthroscopic partial repair and shoulder arthroplasty since it costs less than both options and increases effectiveness by 0.06 and 0.10 quality-adjusted life years (QALYs), respectively. While conservative treatment is the least costly management strategy, subacromial spacer results in a gain of 0.05 QALYs for the additional cost of 522 €, resulting in an ICER of 10,440 €/QALY gain, which is below the standard willingness to pay ratio of $50,000 USD. Strategies with an ICER of less than 50,000 USD are considered to be cost-effective.
Conclusions: Based on the available evidence and reasonably conservative assumptions, subacromial spacer is likely to provide a safe, effective, and cost-effective option for patients with massive IRCTs. Furthermore, this cost-effectiveness analysis may ultimately serve as a guide for development of health care system and insurer policy as well as clinical practice.
Keywords: Biodegradable balloon; Cost-effectiveness; Irreparable tears; Rotator cuff tear; Rotator cuff tear treatment modalities; Subacromial spacer.
Conflict of interest statement
Castagna A. is a company consultant in OrthoSpace. Maman E. serves as OrthoSpace consultant, is a member of the company Scientific Advisory Team, and holds stock options of the company. Brooks EA. is a company consultant in OrthoSpace. Raffaele Garofalo and Alisha C. Gray have no conflict of interest.
Figures
References
-
- Longo UG, Berton A, Papapietro N, Maffulli N, Denaro V. Epidemiology, genetics and biological factors of rotator cuff tears. Med Sport Sci. 2012;57:1–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
