

Primary Ciliary Dyskinesia: Longitudinal Study of Lung Disease by Ultrastructure Defect and Genotype
- PMID: 30067075
- PMCID: PMC6353004
- DOI: 10.1164/rccm.201803-0548OC
Primary Ciliary Dyskinesia: Longitudinal Study of Lung Disease by Ultrastructure Defect and Genotype
Abstract
Rationale: In primary ciliary dyskinesia, factors leading to disease heterogeneity are poorly understood.
Objectives: To describe early lung disease progression in primary ciliary dyskinesia and identify associations between ultrastructural defects and genotypes with clinical phenotype.
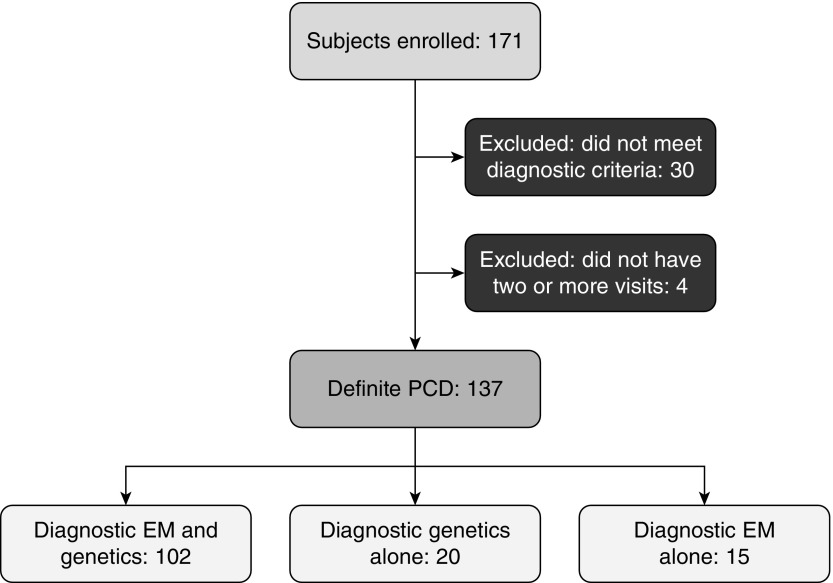
Methods: This was a prospective, longitudinal (5 yr), multicenter, observational study. Inclusion criteria were less than 19 years at enrollment and greater than or equal to two annual study visits. Linear mixed effects models including random slope and random intercept were used to evaluate longitudinal associations between the ciliary defect group (or genotype group) and clinical features (percent predicted FEV1 and weight and height z-scores).
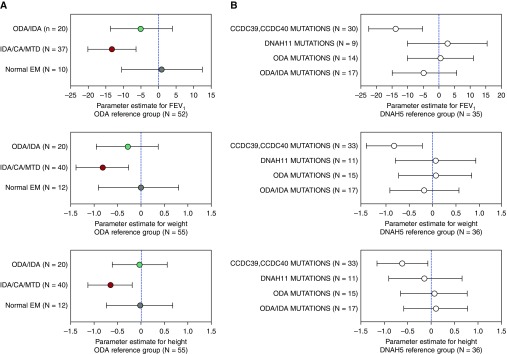
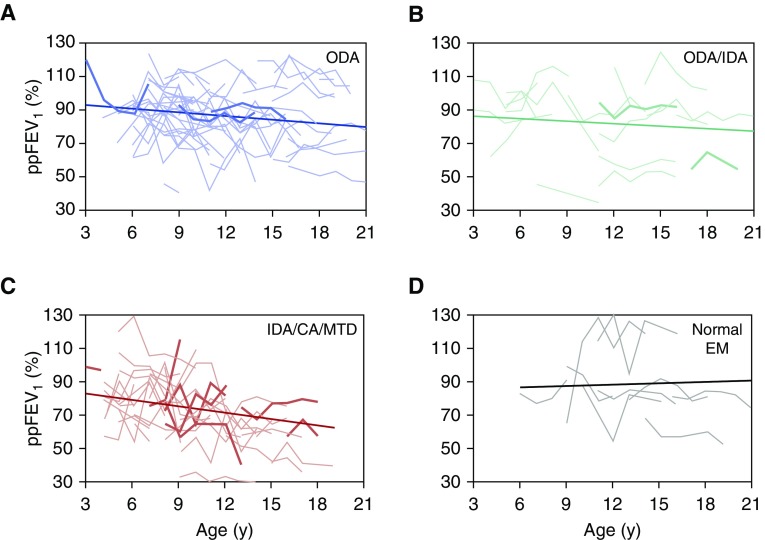
Measurements and main results: A total of 137 participants completed 732 visits. The group with absent inner dynein arm, central apparatus defects, and microtubular disorganization (IDA/CA/MTD) (n = 41) were significantly younger at diagnosis and in mixed effects models had significantly lower percent predicted FEV1 and weight and height z-scores than the isolated outer dynein arm defect (n = 55) group. Participants with CCDC39 or CCDC40 mutations (n = 34) had lower percent predicted FEV1 and weight and height z-scores than those with DNAH5 mutations (n = 36). For the entire cohort, percent predicted FEV1 decline was heterogeneous with a mean (SE) decline of 0.57 (0.25) percent predicted/yr. Rate of decline was different from zero only in the IDA/MTD/CA group (mean [SE], -1.11 [0.48] percent predicted/yr; P = 0.02).
Conclusions: Participants with IDA/MTD/CA defects, which included individuals with CCDC39 or CCDC40 mutations, had worse lung function and growth indices compared with those with outer dynein arm defects and DNAH5 mutations, respectively. The only group with a significant lung function decline over time were participants with IDA/MTD/CA defects.
Keywords: Kartagener syndrome; cilia; respiratory function tests.
Figures
Comment in
-
Rapid Advances in Primary Ciliary Dyskinesia Research. A Brief Update for Pulmonologists.Am J Respir Crit Care Med. 2019 Jan 15;199(2):136-138. doi: 10.1164/rccm.201807-1390ED. Am J Respir Crit Care Med. 2019. PMID: 30110178 No abstract available.
References
-
- Brown DE, Pittman JE, Leigh MW, Fordham L, Davis SD. Early lung disease in young children with primary ciliary dyskinesia. Pediatr Pulmonol. 2008;43:514–516. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
