

Increasing Liver Transplantation Wait-List Dropout for Hepatocellular Carcinoma With Widening Geographical Disparities: Implications for Organ Allocation
- PMID: 30067889
- PMCID: PMC6445639
- DOI: 10.1002/lt.25317
Increasing Liver Transplantation Wait-List Dropout for Hepatocellular Carcinoma With Widening Geographical Disparities: Implications for Organ Allocation
Abstract
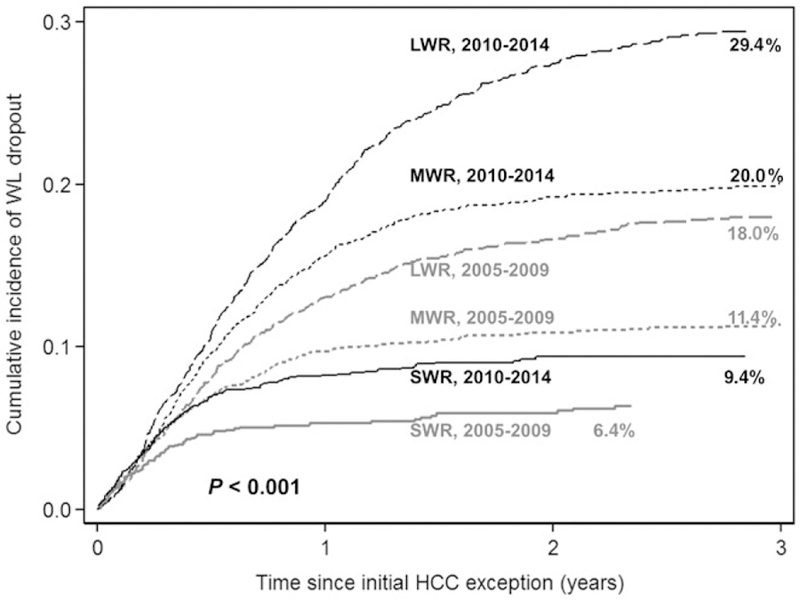
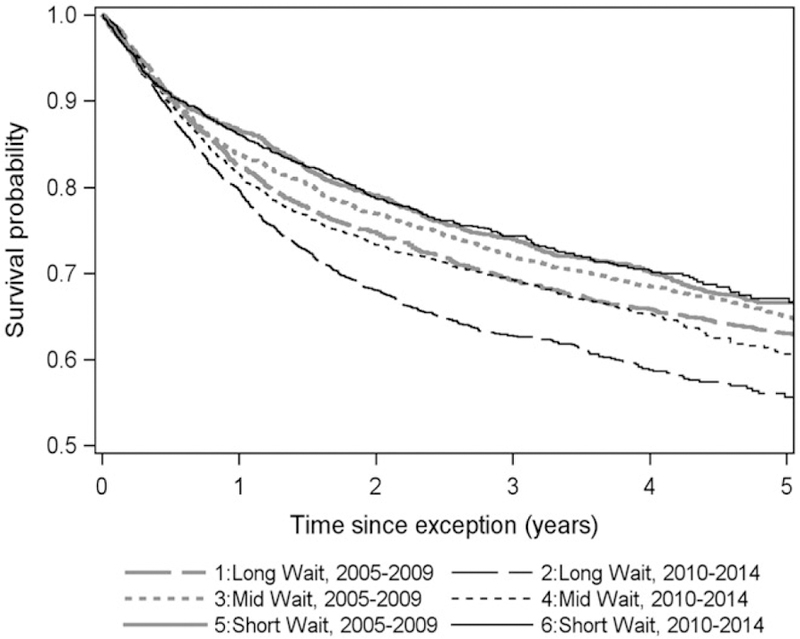
Given the increasing incidence of hepatocellular carcinoma (HCC) and regional variation in liver transplantation (LT) rates for HCC, we investigated temporal and geographic disparities in LT and wait-list dropout. LT candidates receiving Model for End-Stage Liver Disease (MELD) exception from 2005 to 2014 were identified from the United Network for Organ Sharing database (n = 14,320). Temporal differences were compared across 2 eras (2005-2009 and 2010-2014). Regional groups were defined based on median wait time as long-wait region (LWR; regions 1, 5, and 9), mid-wait region (MWR; regions 2, 4, 6, 7, and 8), and short-wait region (SWR; regions 3, 10, and 11). Fine and Gray competing risk regression estimated risk of wait-list dropout as hazard ratios (HRs). The cumulative probability of LT within 3 years was 70% in the LWR versus 81% in the MWR and 91% in the SWR (P < 0.001). From 2005-2009 to 2010-2014, median time to LT increased by 6.0 months (5.6 to 11.6 months) in the LWR compared with 3.8 months (2.6 to 6.4 months) in the MWR and 1.3 months (1.0 to 2.3 months) in the SWR. The cumulative probability of dropout within 3 years was 24% in the LWR versus 16% in the MWR and 8% in the SWR (P < 0.001). From 2005-2009 to 2010-2014, the LWR also had the greatest increase in probability of dropout. Risk of dropout was increased in the LWR (HR, 3.5; P < 0.001) and the MWR (HR, 2.2; P < 0.001) compared with the SWR, and year of MELD exception 2010-2014 (HR, 1.9; P < 0.001) compared with 2005-2009. From 2005-2009 to 2010-2014, intention-to-treat 3-year survival decreased from 69% to 63% in the LWR (P < 0.001), 72% to 69% in the MWR (P = 0.008), and remained at 74% in the SWR (P = 0.48). In conclusion, we observed a significant increase in wait-list dropout in HCC patients in recent years that disproportionately impacted LWR patients. Widening geographical disparities call for changes in allocation policy as well as enhanced efforts at increasing organ donation and utilization.
© 2018 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Potential conflict of interest: Nothing to report.
Figures
References
-
- Wiesner RH, Freeman RB, Mulligan DC. Liver transplantation for hepatocellular cancer: the impact of the MELD allocation policy. Gastroenterology 2004;127(suppl 1):S261–S267. - PubMed
-
- Volk ML. Unfair priority for HCC: A problem whose ideal solution remains unsolved. Am J Transplant 2010;10:1507–1508. - PubMed
-
- Washburn K, Edwards E, Harper A, Freeman R. Hepatocellular carcinoma patients are advantaged in the current liver transplant allocation system. Am J Transplant 2010;10:1643–1648. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
