

Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: a systematic review
- PMID: 30068326
- PMCID: PMC6090960
- DOI: 10.1186/s12913-018-3376-3
Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: a systematic review
Abstract
Background: Healthcare systems internationally are under an ever-increasing demand for services that must be delivered in an efficient, effective and affordable manner. Several patient-related and organisational factors influence health-care expenditure and utilisation, including oropharyngeal dysphagia. Here, we present a systematic review of the literature and meta-analyses investigating how oropharyngeal dysphagia influences healthcare utilisation through length of stay (LOS) and cost.
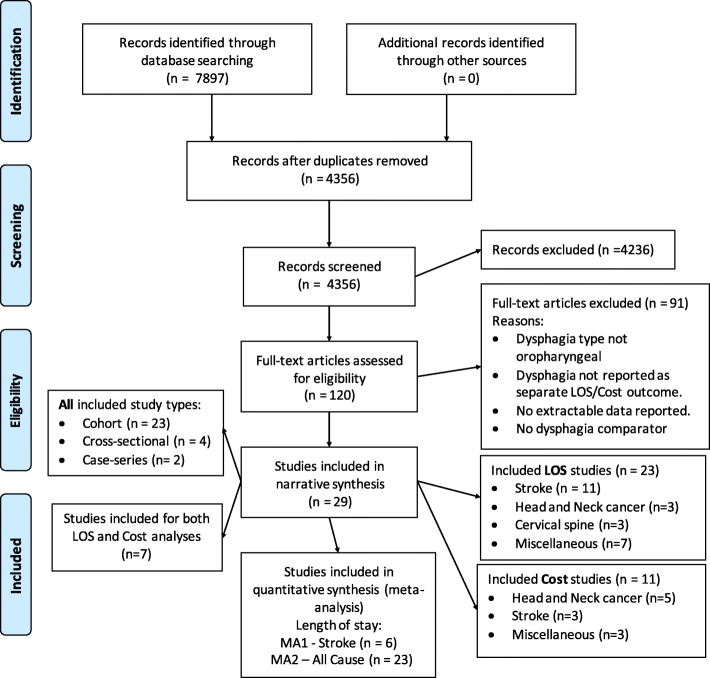
Methods: Using a standardised approach, eight databases were systematically searched for relevant articles reporting on oropharyngeal dysphagia attributable inpatient LOS and healthcare costs through June 2016. Study methodologies were critically appraised and where appropriate, extracted LOS data were analysed in an overall summary statistic.
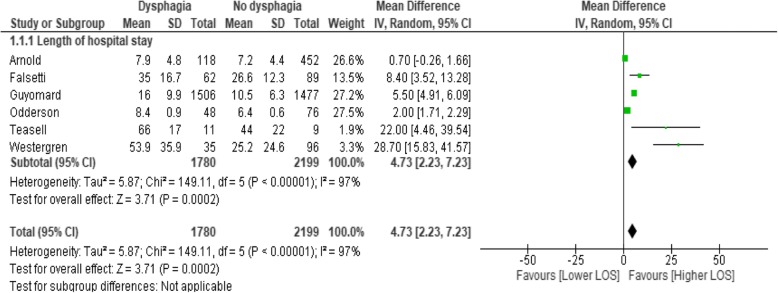
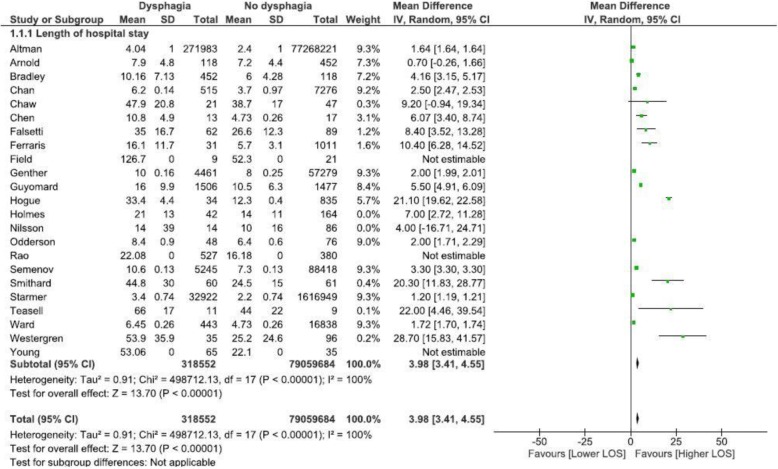
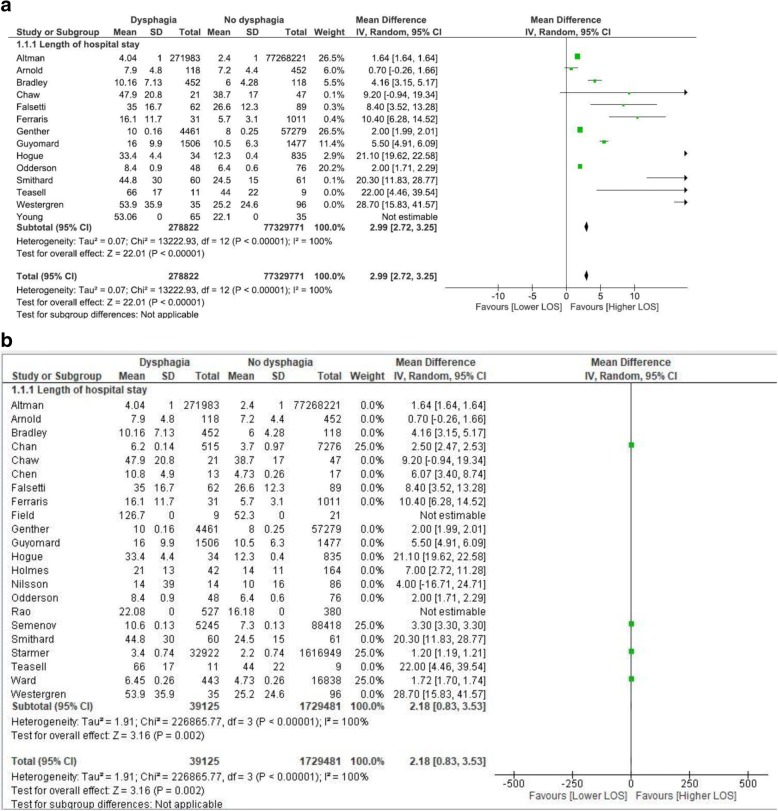
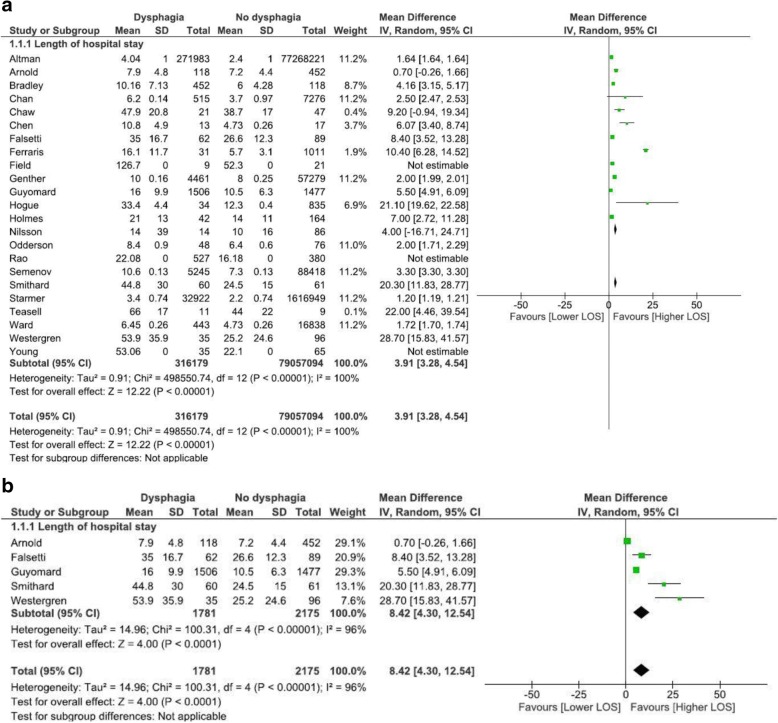
Results: Eleven studies reported on cost data, and 23 studies were included reporting on LOS data. Descriptively, the presence of dysphagia added 40.36% to health care costs across studies. Meta-analysis of all-cause admission data from 13 cohort studies revealed an increased LOS of 2.99 days (95% CI, 2.7, 3.3). A subgroup analysis revealed that admission for stroke resulted in higher and more variable LOS of 4.73 days (95% CI, 2.7, 7.2). Presence of dysphagia across all causes was also statistically significantly different regardless of geographical location: Europe (8.42 days; 95% CI, 4.3; 12.5), North America (3.91 days; 95% CI, 3.3, 4.5). No studies included in meta-analysis were conducted in Asia.
Conclusions: This systematic review demonstrated that the presence of oropharyngeal dysphagia significantly increases healthcare utilisation and cost, highlighting the need to recognise oropharyngeal dysphagia as an important contributor to pressure on healthcare systems.
Keywords: Costs; Expenditure; Financial; Meta-analysis; Swallowing.
Conflict of interest statement
Not applicable.
Not applicable.
The Authors declare that they have no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- National Institute for Health and Care Excellence. Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over. UK; 2016. - PubMed
-
- Stroke Foundation. Clinical Guidelines for Stroke Management 2017. Melbourne Australia. Retrieved from: https://informme.org.au/en/Guidelines/Clinical-Guidelines-for-Stroke-Man....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
