

Precision medicine in COPD: where are we and where do we need to go?
- PMID: 30068688
- PMCID: PMC6156790
- DOI: 10.1183/16000617.0022-2018
Precision medicine in COPD: where are we and where do we need to go?
Abstract
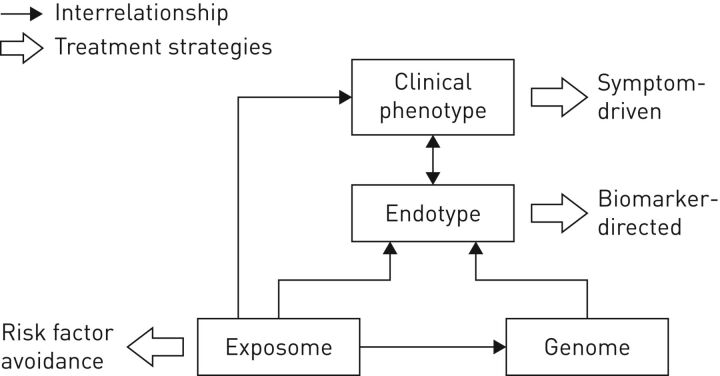
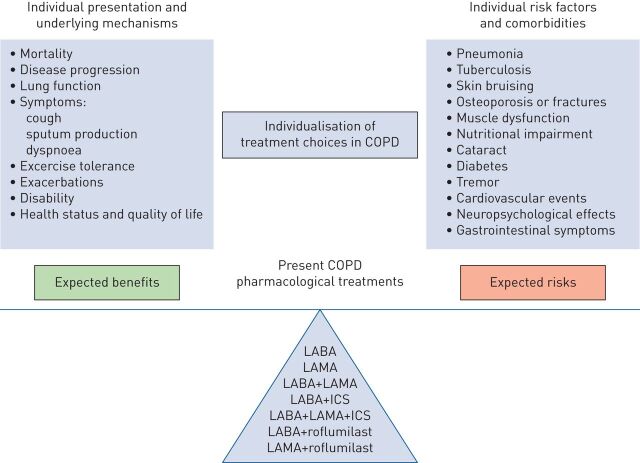
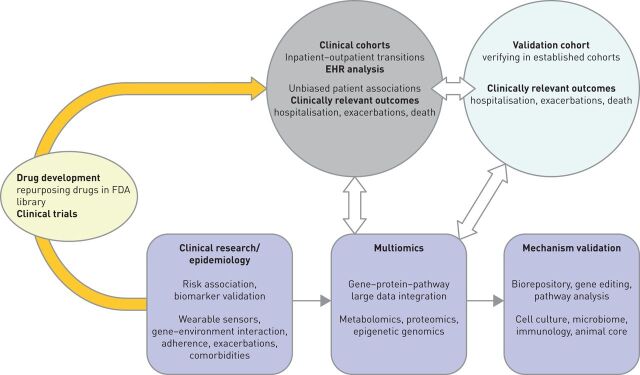
Chronic obstructive pulmonary disease (COPD) was the fourth leading cause of death worldwide in 2015. Current treatments for patients ease discomfort and help decrease disease progression; however, none improve lung function or change mortality. COPD is heterogeneous in its molecular and clinical presentation, making it difficult to understand disease aetiology and define robust therapeutic strategies. Given the complexity of the disease we propose a precision medicine approach to understanding and better treating COPD. It is possible that multiOMICs can be used as a tool to integrate data from multiple fields. Moreover, analysis of electronic medical records could aid in the treatment of patients and in the predictions of outcomes. The Precision Medicine Initiative created in 2015 has made precision medicine approaches to treat disease a reality; one of these diseases being COPD.
Copyright ©ERS 2018.
Conflict of interest statement
Conflict of interest: F.J. Martinez reports personal fees and non-financial support from the American College of Chest Physicians (personal fee honoraria and non-personal travel support for COPD CME programmes in India), personal fees and non-financial support from AstraZeneca (personal fees and non-personal travel support for COPD advisory boards, a study steering committee and an ALAT presentation), personal fees and non-financial support from Boehringer Ingelheim (personal fees and non-personal travel support for a COPD advisory board, and personal fees for an ATS presentation), non-financial support from ProterrixBio (support for an NIH study, but no direct financial compensation for a COPD scientific advisory board), personal fees and non-financial support from Continuing Education (personal fee honorarium and non-personal travel support for a cough CME programme), personal fees from Columbia University, Haymarket Communications, Integritas, Methodist Hospital Brooklyn, New York University, UpToDate, WebMD/MedScape and Western Connecticut Health Network (personal fee honoraria for COPD CME programmes), personal fees and non-financial support from ConCert, Pearl Pharmaceuticals, Roche, Sunovion and Theravance (personal fee honoraria and non-personal travel support for COPD advisory boards), personal fees and non-financial support from Genentech (personal fee and non-personal travel support for a COPD advisory board and non-financial support for an asthma data safety monitoring board), personal fees and non-financial support from GlaxoSmithKline (personal fee honoraria and non-personal travel support for COPD advisory boards, non-personal travel support for a study steering committee and an ERS presentation, and academic co-authorship for a data safety monitoring board), personal fees and non-financial support from Inova Fairfax Health System, Miller Communications, the National Association for Continuing Education, PeerView Communications, Prime Communications, the Puerto Rican Respiratory Society and Chiesi (personal fee honoraria and non-personal travel support for COPD CME programmes), personal fees from Inthought Research (personal fee honoraria for a COPD/asthma teleconference), personal fees from MD Magazine (personal fee honorarium and non-personal travel support for a COPD CME programme), personal fees and non-financial support from Novartis (personal fees honoraria and non-personal travel support for a COPD advisory board and international meeting COPD disease presentations), personal fees from Unity (personal fee honoraria for a COPD teleconference), personal fees from the American Thoracic Society (personal fee honoraria for being deputy editor of the AJRCCM), and a grant from the National Institutes of Health (COPD UO1/RO1).
Figures
Comment in
References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Arch Bronconeumol 2017; 53: 128–149. - PubMed
-
- Faner R, Agustí A. Multilevel, dynamic chronic obstructive pulmonary disease heterogeneity. A challenge for personalized medicine. Ann Am Thorac Soc 2016; 13: Suppl. 5, S466–S470. - PubMed
-
- Agustí A, Bafadhel M, Beasley R, et al. Precision medicine in airway diseases: moving to clinical practice. Eur Respir J 2017; 50: 1701655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical