

Premature Clinical Trial Discontinuation in the Era of Immune Checkpoint Inhibitors
- PMID: 30068783
- PMCID: PMC6292544
- DOI: 10.1634/theoncologist.2018-0003
Premature Clinical Trial Discontinuation in the Era of Immune Checkpoint Inhibitors
Abstract
Background: Clinical trial completion is critical for new cancer therapies. Premature trial termination or withdrawal is common and impairs progress. We assessed factors of early terminated/withdrawn oncology trials focusing on trials with immune checkpoint inhibitors (ICI), hypothesizing that the latter may be associated with lower rates of premature discontinuation.
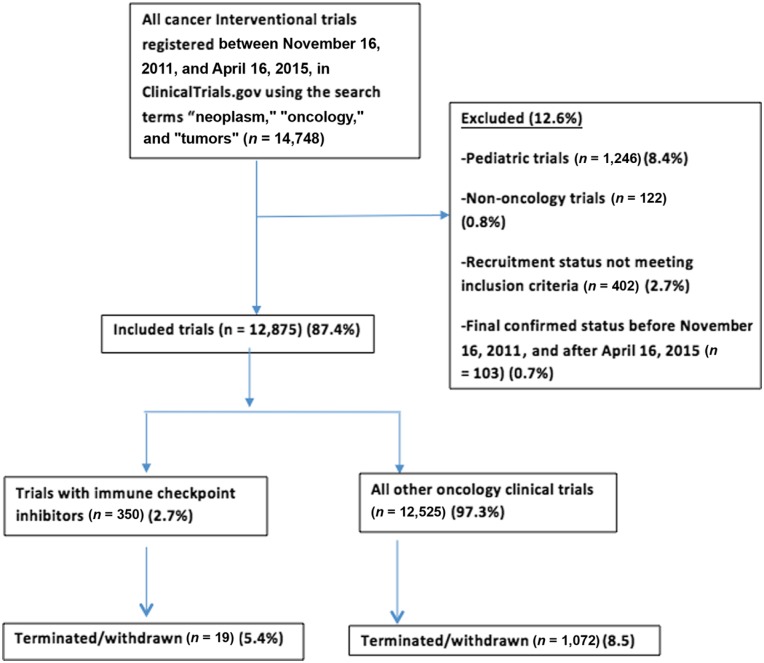
Materials and methods: We reviewed all adult, intervention, oncology trials registered in ClinicalTrials.gov (November 16, 2011, to April 16, 2015) to identify all terminated/withdrawn trials and reasons for termination. Logistics regression model was used to identify factors associated with early termination/withdrawal. Discontinuation rate was compared in trials with and without ICI.
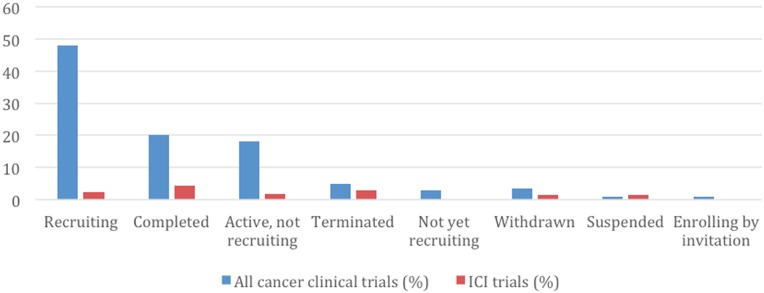
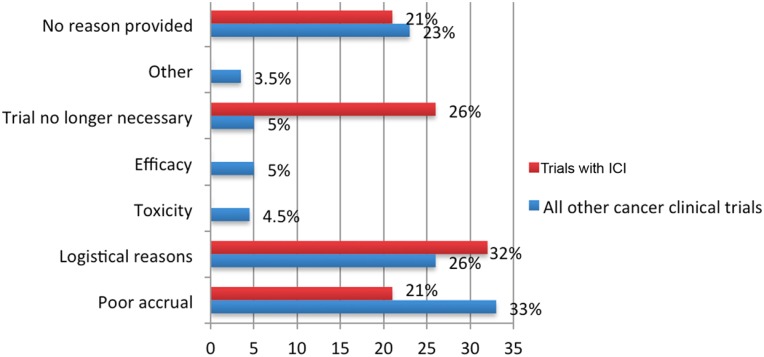
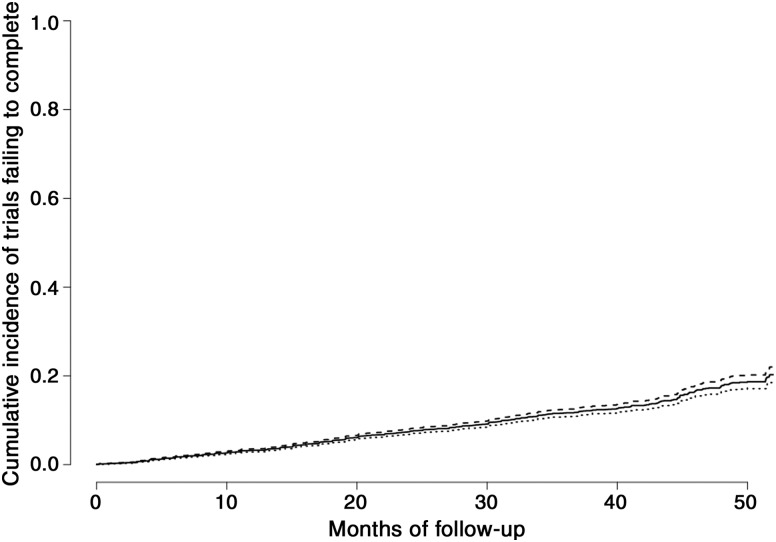
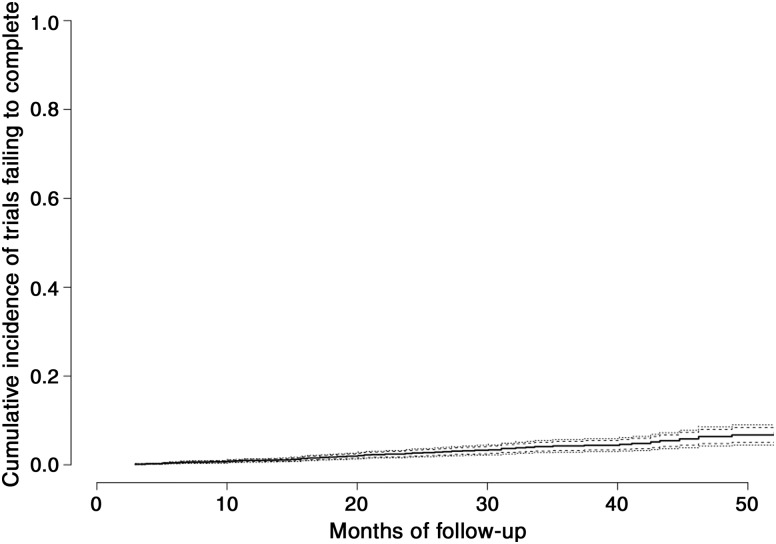
Results: We identified 12,875 trials (35% industry funded, 12% federal funded), of which 8.5% were prematurely terminated (5%) or withdrawn (3.5%); the main reasons were poor accrual (33%) and logistical (24%). ICI trials (n = 350) had a nonsignificant lower rate of termination or withdrawal compared with all other oncology trials (5.4% vs. 8.5%; p = .9) and were less likely to discontinue due to poor accrual (nonsignificant difference: 21% vs. 33%; p = .4). ICI trials were also less likely to discontinue compared with all other oncology drug trials (e.g., chemotherapy, targeted inhibitors, antiangiogenesis, biologics; 5.4% vs. 7.9%, respectively, nonsignificant difference). The 4-year cumulative incidence of failing to complete for reasons unrelated to toxicity or efficacy was 18% (95% confidence interval 16%-20%). There was no association between annual incidence across different tumor types or accrual goal and rate of trial termination.
Conclusion: Poor accrual represents the main cause of early cancer trial termination. Premature termination/withdrawal rate was not significantly lower in ICI compared with other trials. Clinical trial completion remains a high priority and can be influenced by provider and patient factors.
Implications for practice: Clinical trial completion is critical for new cancer therapies. Premature trial termination or withdrawal is common and impairs progress. This study assessed factors of early terminated/withdrawn oncology trials, focusing on trials with immune checkpoint inhibitors (ICI), and found that poor accrual represents the main cause of early cancer trial termination. Premature termination/withdrawal rate was not significantly lower in immune checkpoint inhibitor trials compared to other trials. The discussion herein is focused on measures taken by the National Cancer Institute and other institutions to improve clinical trial accrual and prevent premature clinical trial discontinuation.
Keywords: Cancer; Clinical research; Clinical trial termination; Immune checkpoint inhibitors; Immunotherapy.
© AlphaMed Press 2018.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
