

Linked dimensions of psychopathology and connectivity in functional brain networks
- PMID: 30068943
- PMCID: PMC6070480
- DOI: 10.1038/s41467-018-05317-y
Linked dimensions of psychopathology and connectivity in functional brain networks
Abstract
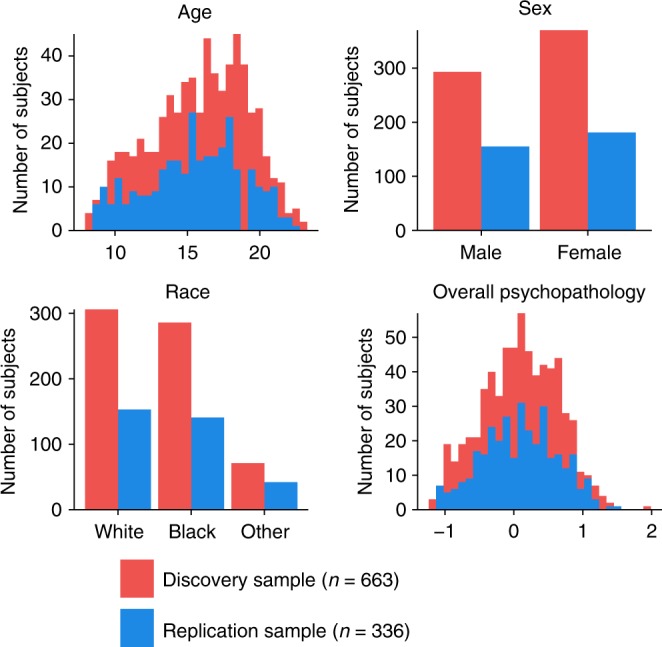
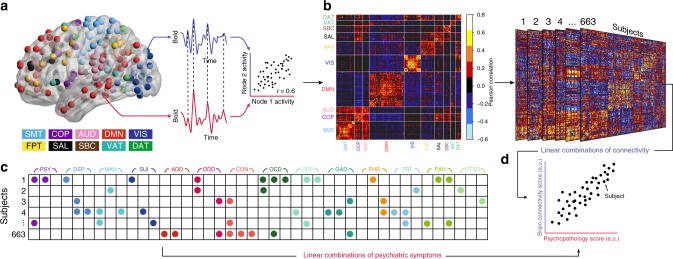
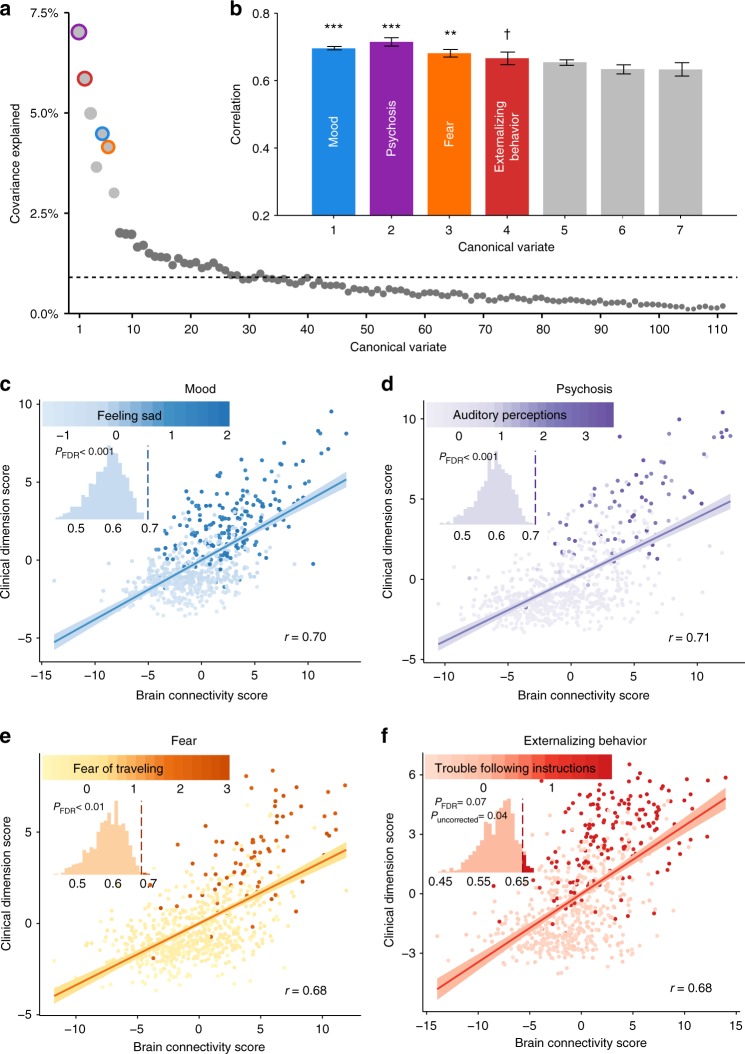
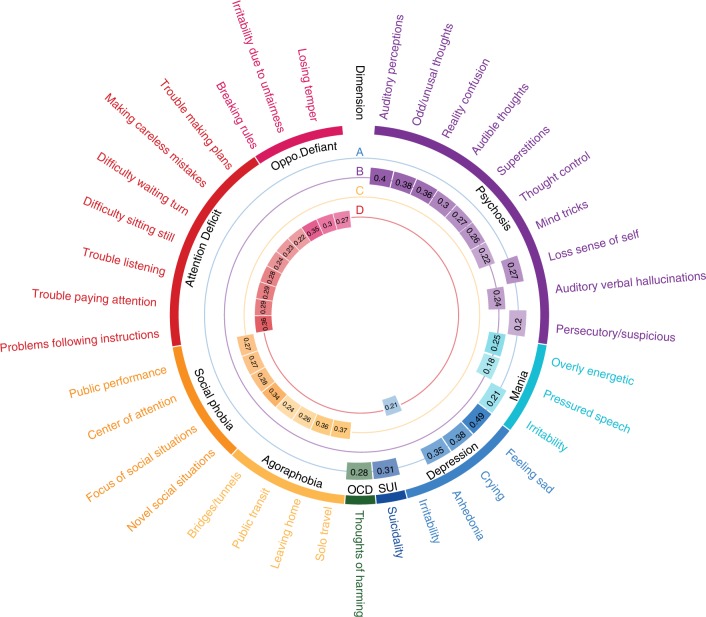
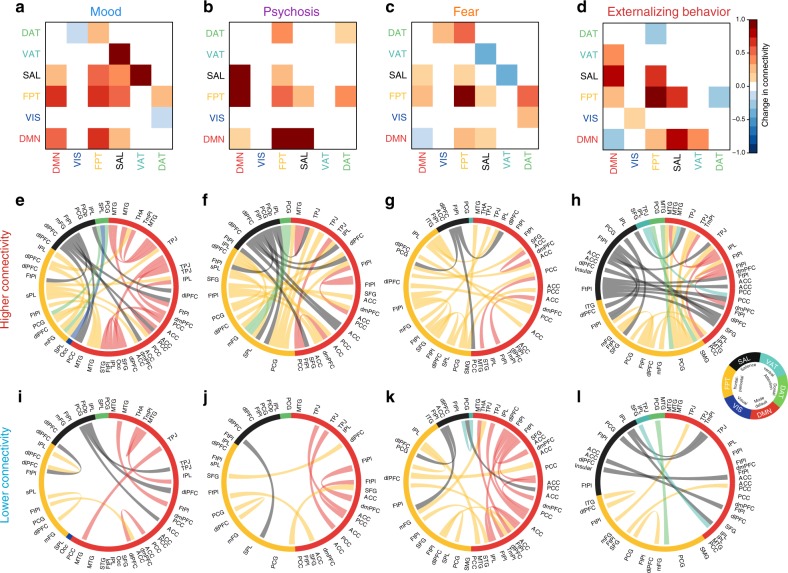
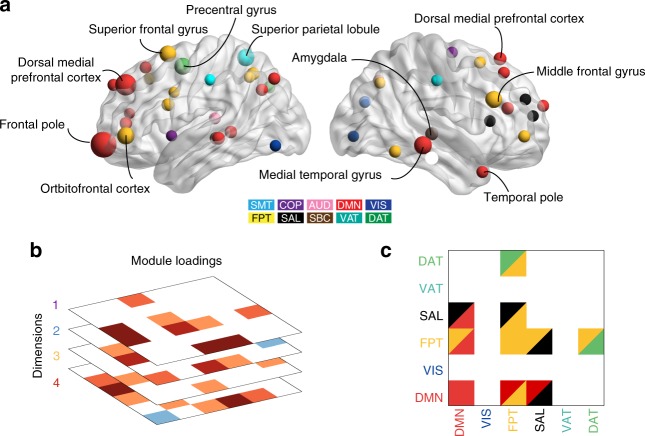
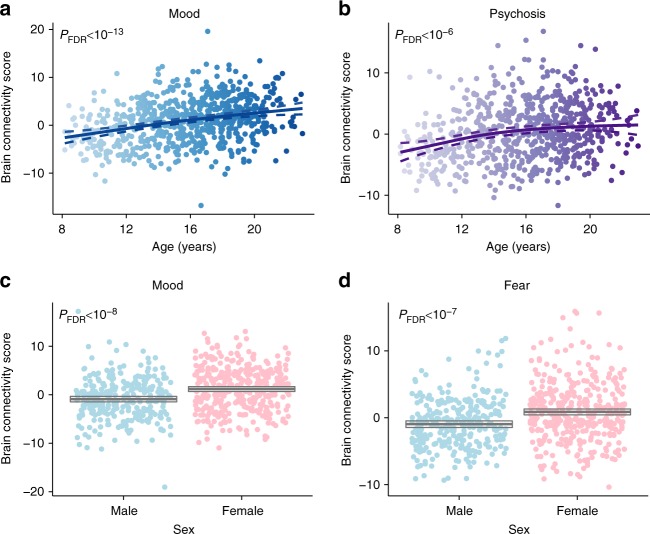
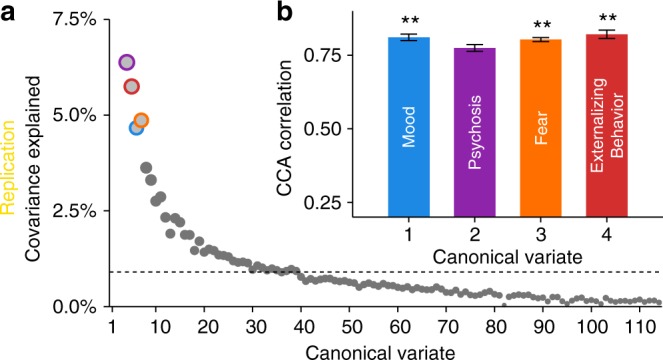
Neurobiological abnormalities associated with psychiatric disorders do not map well to existing diagnostic categories. High co-morbidity suggests dimensional circuit-level abnormalities that cross diagnoses. Here we seek to identify brain-based dimensions of psychopathology using sparse canonical correlation analysis in a sample of 663 youths. This analysis reveals correlated patterns of functional connectivity and psychiatric symptoms. We find that four dimensions of psychopathology - mood, psychosis, fear, and externalizing behavior - are associated (r = 0.68-0.71) with distinct patterns of connectivity. Loss of network segregation between the default mode network and executive networks emerges as a common feature across all dimensions. Connectivity linked to mood and psychosis becomes more prominent with development, and sex differences are present for connectivity related to mood and fear. Critically, findings largely replicate in an independent dataset (n = 336). These results delineate connectivity-guided dimensions of psychopathology that cross clinical diagnostic categories, which could serve as a foundation for developing network-based biomarkers in psychiatry.
Conflict of interest statement
R.T.S. has received legal consulting and advisory board income from Genentech/Roche. All other authors (C.H.X., Z.M., R.C., S.G., R.F.B., A.N.K., M.E.C., P.A.C., A.G., S.V., Z.C., T.M.M., D.R.R., K.R., D.H.W., C.D., R.C.G., R.E.G., D.S.B., and T.D.S.) declare no competing interest.
Figures
References
Publication types
MeSH terms
Grants and funding
- R01MH107235/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- P50 MH096891/MH/NIMH NIH HHS/United States
- R01 EB022573/EB/NIBIB NIH HHS/United States
- R01 MH112847/MH/NIMH NIH HHS/United States
- R01MH101111/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- R01 NS099348/NS/NINDS NIH HHS/United States
- R01 MH107235/MH/NIMH NIH HHS/United States
- P50MH096891/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- R01 DC009209/DC/NIDCD NIH HHS/United States
- K08 MH079364/MH/NIMH NIH HHS/United States
- R21 MH106799/MH/NIMH NIH HHS/United States
- R01 MH101111/MH/NIMH NIH HHS/United States
- K08MH079364/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- R01EB022573/U.S. Department of Health & Human Services | NIH | National Institute of Biomedical Imaging and Bioengineering (NIBIB)/International
- RC2 MH089924/MH/NIMH NIH HHS/United States
- R01 MH113550/MH/NIMH NIH HHS/United States
- K01 MH102609/MH/NIMH NIH HHS/United States
- R21MH106799/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- R01 HD086888/HD/NICHD NIH HHS/United States
- MH089983/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- R01MH112847/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- MH089924/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- U54 HD086984/HD/NICHD NIH HHS/United States
- K01MH102609/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- R01MH107703/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)/International
- R01 NS085211/NS/NINDS NIH HHS/United States
- R01NS085211/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)/International
- R01 MH107703/MH/NIMH NIH HHS/United States
- RC2 MH089983/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
