

Effect of pneumoperitoneum and steep reverse-Trendelenburg position on mean systemic filling pressure, venous return, and microcirculation during esophagectomy
- PMID: 30069335
- PMCID: PMC6051808
- DOI: 10.21037/jtd.2018.05.169
Effect of pneumoperitoneum and steep reverse-Trendelenburg position on mean systemic filling pressure, venous return, and microcirculation during esophagectomy
Abstract
Background: Keeping adequate tissue perfusion during high-risk abdominal surgery is of utmost importance to decrease postoperative complications. The objective was to investigate the alteration in mean systemic filling pressure (MSFP), venous return (VR) and sublingual microcirculation during pneumoperitoneum and steep reverse-Trendelenburg position during thoracolaparoscopic esophagectomy.
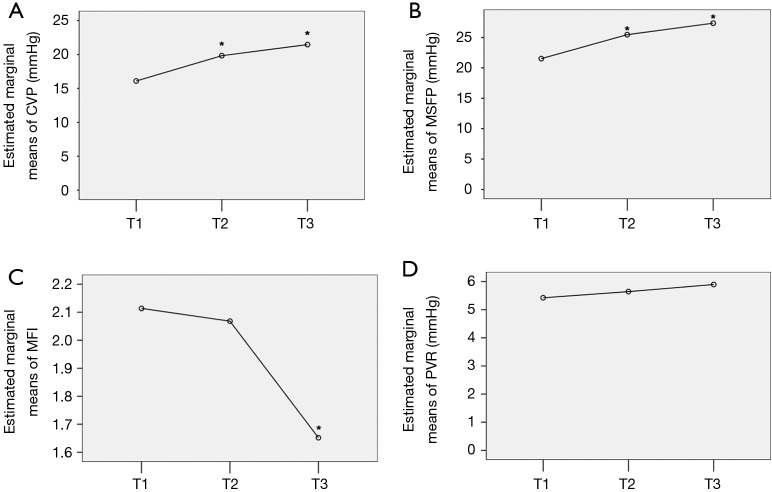
Methods: This is a single-center prospective observational study in operating room at a university hospital. Eleven consecutive patients undergoing minimally invasive esophagectomy. Intraoperative hemodynamic and sublingual microcirculatory variables were simultaneously measured within 5 minutes at the following time points: T1, baseline supine position before the start of surgery; T2, pneumoperitoneum in supine position; T3, steep reverse-Trendelenburg position after the pneumoperitoneum. The cardiac output (CO) was obtained with continuous pulse contour waveform-derived measurements, and the MSFP was estimated with the analogue method.
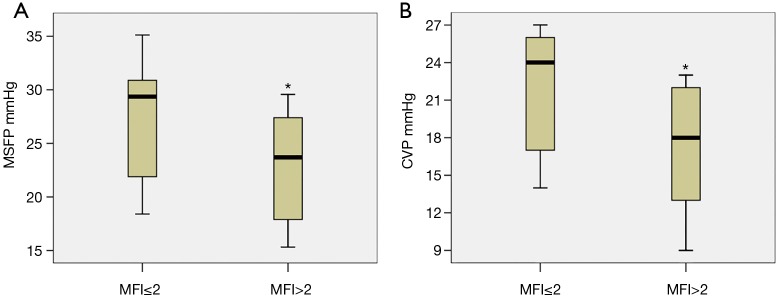
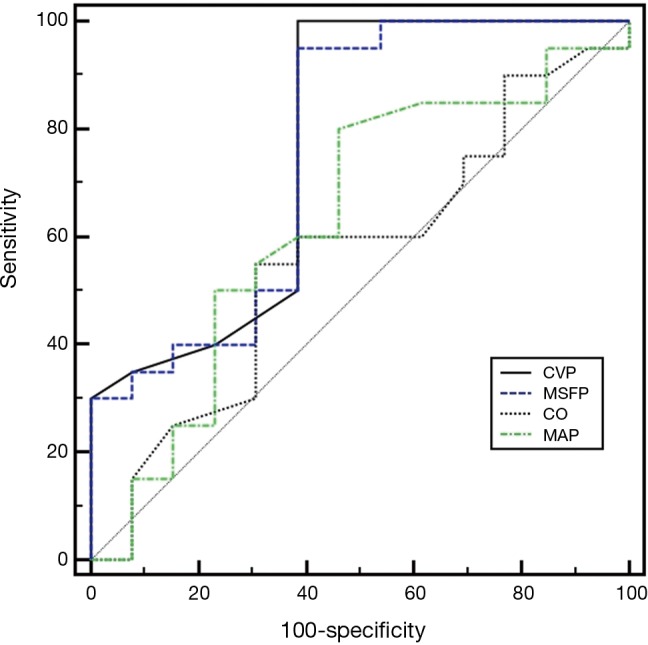
Results: The pneumoperitoneum and reverse-Trendelenburg caused an increase in stroke volume variation (SVV), MSFP and central venous pressure (CVP), and a decrease in the microcirculatory perfusion index (MFI, <0.05). However, changes in CO, pressure gradient of VR, resistance of VR and blood pressure were not consistent and did not differ significantly across timepoints. Moreover, MFI is significantly related to CVP and MSFP but not to CO and blood pressure (BP). Measurements with MFI ≤2 have a higher CVP and MSFP compared to those with MFI >2. Using a CVP ≥23 mmHg to detect MFI ≤2 results in a sensitivity of 61.54% and a specificity of 100%.
Conclusions: A high CVP is related to poor microcirculatory flow perfusion even if the macrocirculation has been maintained during pneumoperitoneum.
Keywords: Microcirculation; central venous pressure (CVP); esophageal surgery; minimally-invasive laparoscopy.
Conflict of interest statement
Conflicts of Interest: DP Veelo and MW Hollmann have received support [contract was made, under name: quality improvement project, Academic Medical Center (AMC)] from Edwards regarding a different project but for the same patient population. Funders were not involved in any activities regarding this study. DP Veelo, SS Gisbertz and MI van Berge Henegouwen have done consultancy work for Edwards in light of a different project. C Ince has developed SDF imaging and is listed as inventor on related patents commercialized by MicroVision Medical (MVM) under a license from the AMC. He has been a consultant for MVM in the past, but has not been involved with this company for more than 5 years now, except that he still holds shares. The other authors have no conflicts of interest to declare.
Figures

References
-
- Rademaker BM, Odoom JA, de Wit LT, et al. Haemodynamic effects of pneumoperitoneum for laparoscopic surgery: a comparison of CO2 with N2O insufflation. Eur J Anaesthesiol 1994;11:301-6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources