

Fixation of periprosthetic or osteoporotic distal femoral fractures with locking plates: a pilot randomised controlled trial
- PMID: 30069590
- PMCID: PMC6470115
- DOI: 10.1007/s00264-018-4061-1
Fixation of periprosthetic or osteoporotic distal femoral fractures with locking plates: a pilot randomised controlled trial
Abstract
Introduction: We hypothesised that the use of a polyaxial locking plate design offers the same clinical benefits as a monoaxial locking plate system following distal femoral osteoporotic/periprosthetic fracture fixation.
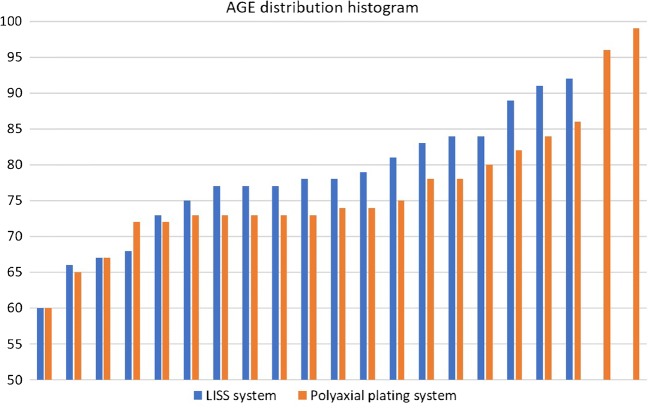
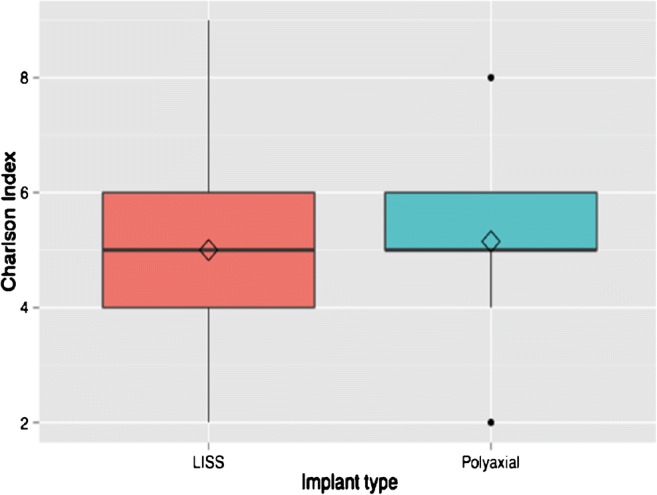
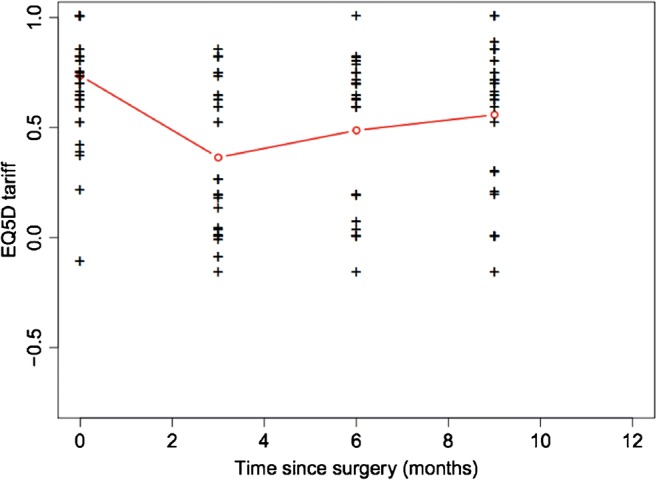
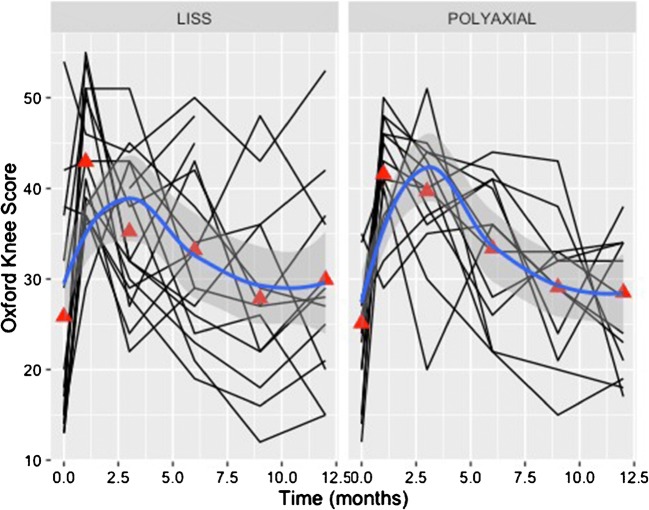
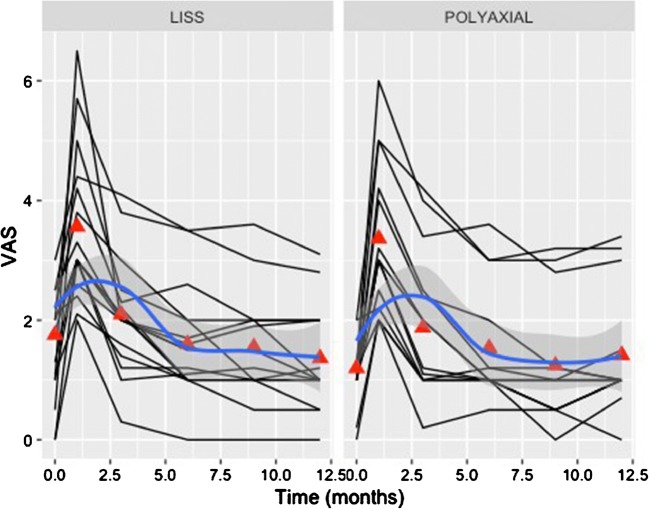
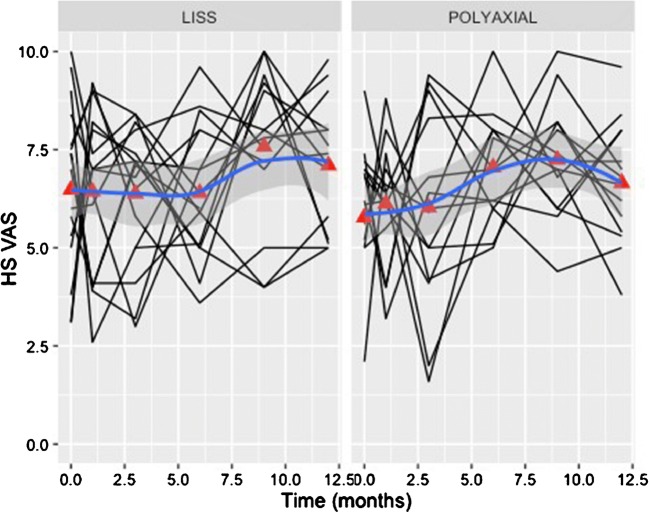
Method: A multicentre prospective randomised pilot trial was conducted. Inclusion criteria were patients over 60 years with a displaced osteoporotic or periprosthetic distal femoral fracture. Details documented included time to union, complications, reinterventions and functional outcomes according to the Oxford knee score and EuroQol EQ-5D. Analysis of factors influencing an early fracture healing response was performed between those with clear features of radiological callus formation at three months. Statistical analysis was performed using a logistic regression model with multiple covariates assessed for each plate system (1:1 ratio) over a follow-up period of one year.
Results: Forty patients (34 females) with a mean age of 77 (60-99) were recruited. Four patients deceased within the first six months. Twenty-five patients united by the six month follow-up. Six more patients progressed to union between six and nine months. Five patients developed non-union (two patients had implant failure; one in each group) and all underwent revision surgery. Malunion was evident in two cases, one with 15° of valgus (monoaxial plate), and one with 12° of recurvatum (polyaxial plate). Between the two plate systems, statistical analysis revealed no significant differences in most of the recorded parameters. Radiological features of early bone healing were present when the surgical approach was smaller (p = 0.015), and when a greater working length of the bridging plate was present (p = 0.016).
Conclusion: Both plate systems demonstrated good union rates and limited implant related complications. Good reduction, mechanically sound construct and respect of the local fracture biology was more important than the particular plate design characteristics.
Keywords: Femoral fracture; Locking plate; Periprosthetic fracture; Polyaxial.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Schatzker J, Lambert DC. Supracondylar fractures of the femur. Clin Orthop Relat Res. 1979;138:77–83. - PubMed
-
- Pape HC, Hildebrand F, Pertschy S, Zelle B, Garapati R, Grimme K, Krettek C, Reed RL., 2nd Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery. J Trauma. 2002;53(3):452–461. doi: 10.1097/00005373-200209000-00010. - DOI - PubMed
-
- Haidukewych GJ, Jacofsky DJ, Hanssen AD. Treatment of periprosthetic fractures around a total knee arthroplasty. J Knee Surg. 2003;16(2):111–117. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
