

Muscular Dystrophy Surveillance, Tracking, and Research Network pilot: Population-based surveillance of major muscular dystrophies at four U.S. sites, 2007-2011
- PMID: 30070776
- PMCID: PMC6265066
- DOI: 10.1002/bdr2.1371
Muscular Dystrophy Surveillance, Tracking, and Research Network pilot: Population-based surveillance of major muscular dystrophies at four U.S. sites, 2007-2011
Abstract
Background: For 10 years, the Muscular Dystrophy Surveillance, Tracking, and Research Network (MD STARnet) conducted surveillance for Duchenne and Becker muscular dystrophy (DBMD). We piloted expanding surveillance to other MDs that vary in severity, onset, and sources of care.
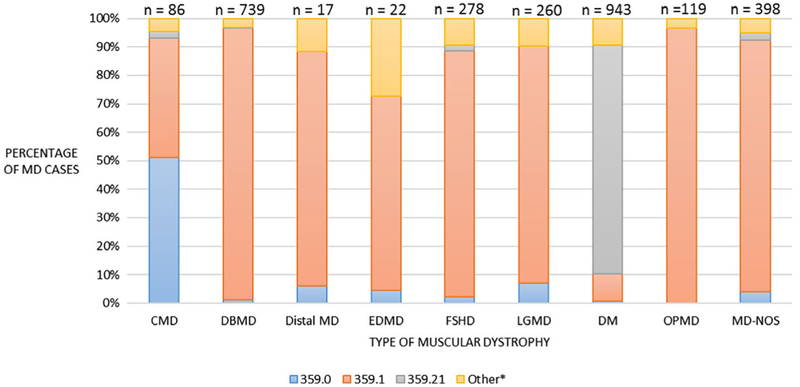
Methods: Our retrospective surveillance included individuals diagnosed with one of nine eligible MDs before or during the study period (January 2007-December 2011), one or more health encounters, and residence in one of four U.S. sites (Arizona, Colorado, Iowa, or western New York) at any time within the study period. We developed case definitions, surveillance protocols, and software applications for medical record abstraction, clinical review, and data pooling. Potential cases were identified by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 359.0, 359.1, and 359.21 and International Classification of Diseases, Tenth Revision (ICD-10) codes G71.0 and G71.1. Descriptive statistics were compared by MD type. Percentage of MD cases identified by each ICD-9-CM code was calculated.
Results: Of 2,862 cases, 32.9% were myotonic, dystrophy 25.8% DBMD, 9.7% facioscapulohumeral MD, and 9.1% limb-girdle MD. Most cases were male (63.6%), non-Hispanic (59.8%), and White (80.2%). About, half of cases were genetically diagnosed in self (39.1%) or family (6.2%). About, half had a family history of MD (48.9%). The hereditary progressive MD code (359.1) was the most common code for identifying eligible cases. The myotonic code (359.21) identified 83.4% of eligible myotonic dystrophy cases (786/943).
Conclusions: MD STARnet is the only multisite, population-based active surveillance system available for MD in the United States. Continuing our expanded surveillance will contribute important epidemiologic and health outcome information about several MDs.
Keywords: Clinical Modification (ICD-9-CM) codes; International Classification of Diseases; MD STARnet; Ninth Revision; active surveillance; medical record abstraction; muscular dystrophies; population-based.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
CONFLICT OF INTEREST
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Andrews JG, Soim A, Pandya S, Westfield CP, Ciafaloni E, Fox DJ, Birnkrant DJ, Cunniff CM, Sheehan DW. (2016). Respiratory care received by individuals with Duchenne muscular dystrophy from 2000 to 2011. Respiratory Care 61 (10):1349–1359. doi: https://doi.org/10.4187/respcare.04676 - DOI - PubMed
-
- Caspers Conway K, Mathews KD, Paramsothy P, Oleszek J, Trout C, Zhang Y, Romitti PA. (2015). Neurobehavioral concerns among males with dystrophinopathy using population-based surveillance data from the Muscular Dystrophy Surveillance, Tracking, and Research Network. Journal of Developmental and Behavioral Pediatrics 36(6):455–463. doi: https://doi.org/10.1097/DBP.0000000000000177 - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention. (2009). Prevalence of Duchenne/-Becker muscular dystrophy among males aged 5-24 years—Four states, 2007. Morbidity and Mortality Weekly Report 58(40):1119–1122. - PubMed
-
- Ciafaloni E, Kumar A, Liu K, Pandya S, Westfield C, Fox DJ, Caspers Conway KM, Cunniff C, Mathews K, West N, Romitti PA, McDermott MP. (2016). Age at onset of first signs or symptoms predicts age at loss of ambulation in Duchenne and Becker muscular dystrophy: Data from the MD STARnet. Journal of Pediatric Rehabilitation Medicine 9(1):5—11. doi: https://doi.org/10.3233/PRM-160361 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
