

Continuously Updated Estimation of Heart Transplant Waitlist Mortality
- PMID: 30071995
- PMCID: PMC6298792
- DOI: 10.1016/j.jacc.2018.05.045
Continuously Updated Estimation of Heart Transplant Waitlist Mortality
Abstract
Background: Heart transplant allocation in the United States is made on the basis of coarse tiers, defined by mechanical circulatory devices and therapy for advanced heart failure, updated infrequently as a patient's condition deteriorates. Thus, many patients die awaiting heart transplantation. What is needed is a tool that continuously updates risk of mortality as a patient's condition changes to inform clinical decision making.
Objectives: This study sought to develop a decision aid that aggregates adverse events and measures of end-organ function into a continuously updated waitlist mortality estimate.
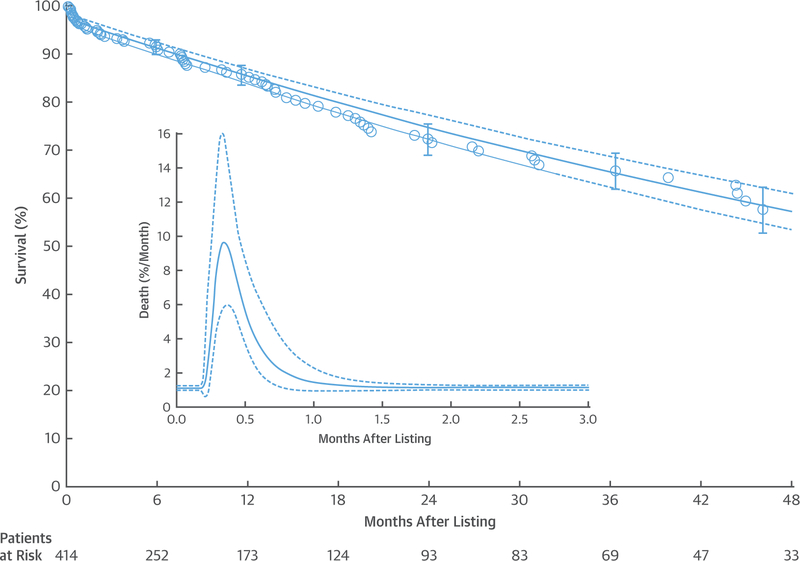
Methods: From 2008 to 2013, 414 patients were listed for heart transplantation at Cleveland Clinic, Cleveland, Ohio. The endpoint was waitlist death. Pre-listing patient characteristics and events and laboratory results during listing were analyzed. At each event or measurement change, mortality was recomputed from the resulting model.
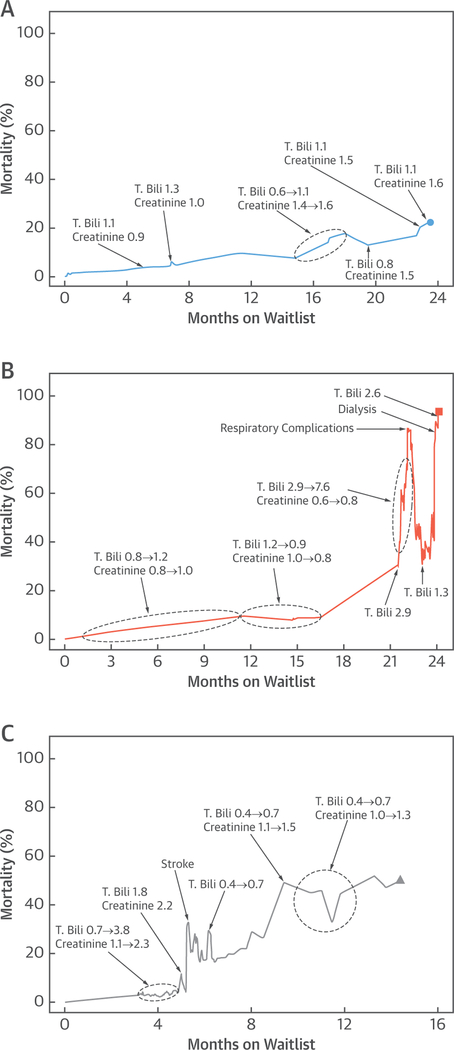
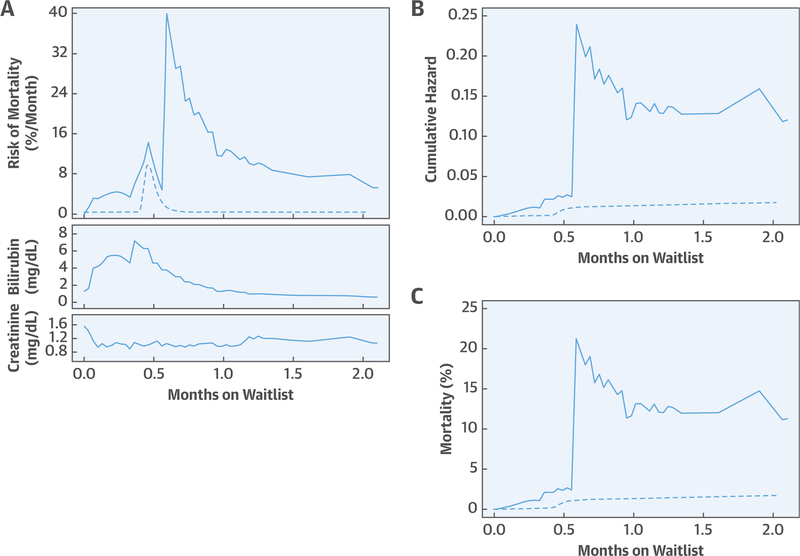
Results: There were 77 waitlist deaths, with 1- and 4-year survival of 85% and 57%, respectively. When time-varying events and measurements were incorporated into a mortality model, pre-listing patient characteristics became nonsignificant. Neurological events (hazard ratio [HR]: 13.5; 95% confidence interval [CI]: 7.63 to 23.8), new requirement for dialysis (HR: 3.67; 95% CI: 1.88 to 7.14), more respiratory complications (HR: 1.79 per episode; 95% CI: 1.23 to 2.59), and higher serum bilirubin (p < 0.0001) and creatinine (p < 0.0001) yielded continuously updated estimates of patient-specific mortality across the waitlist period.
Conclusions: Mortality risk for patients with advanced heart failure who are listed for transplantation is related to adverse events and end-organ dysfunction that change over time. A continuously updated mortality estimate, combined with clinical evaluation, may inform status changes that could reduce mortality on the heart transplant waiting list.
Keywords: heart failure; mathematical modeling; mechanical circulatory support; risk score.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Data Science and Cardiac Surgery: Can We Bridge the Gap Between Innovation and Application?J Am Coll Cardiol. 2018 Aug 7;72(6):660-661. doi: 10.1016/j.jacc.2018.06.007. J Am Coll Cardiol. 2018. PMID: 30071996 No abstract available.
References
-
- U.S. Department of Health and Human Services: Organ Procurement and Transplantation Network. OPTN/UNOS Thoracic Organ Transplantation Committee. Proposal to Modify the Adult Heart Allocation System. 2017. Available at: http://optn.transplant.hrsa.gov/media/1921/thoracic_adult_heart_allocati.... Accessed July 2, 2018.
-
- Lund LH, Edwards LB, Kucheryavaya AY, et al. The Registry of the International Society for Heart and Lung Transplantation: thirty-second official adult heart transplantation report–2015; focus theme: early graft failure. J Heart Lung Transplant 2015;34:1244–54. - PubMed
-
- U.S. Department of Health and Human Services: Organ Procurement and Transplantation Network. Adult Heart Allocation Changes 2016. 2017. Available at: https://optn.transplant.hrsa.gov/governance/public-comment/adult-heart-a.... Accessed July 2, 2018.
-
- U.S. Department of Health and Human Services: Organ Procurement and Transplantation Network. Policies. 2017. Available at: https://optn.transplant.hrsa.gov/governance/policies. Accessed June 13, 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
