

Assessment of ASC specks as a putative biomarker of pyroptosis in myelodysplastic syndromes: an observational cohort study
- PMID: 30072146
- PMCID: PMC6505461
- DOI: 10.1016/S2352-3026(18)30109-1
Assessment of ASC specks as a putative biomarker of pyroptosis in myelodysplastic syndromes: an observational cohort study
Abstract
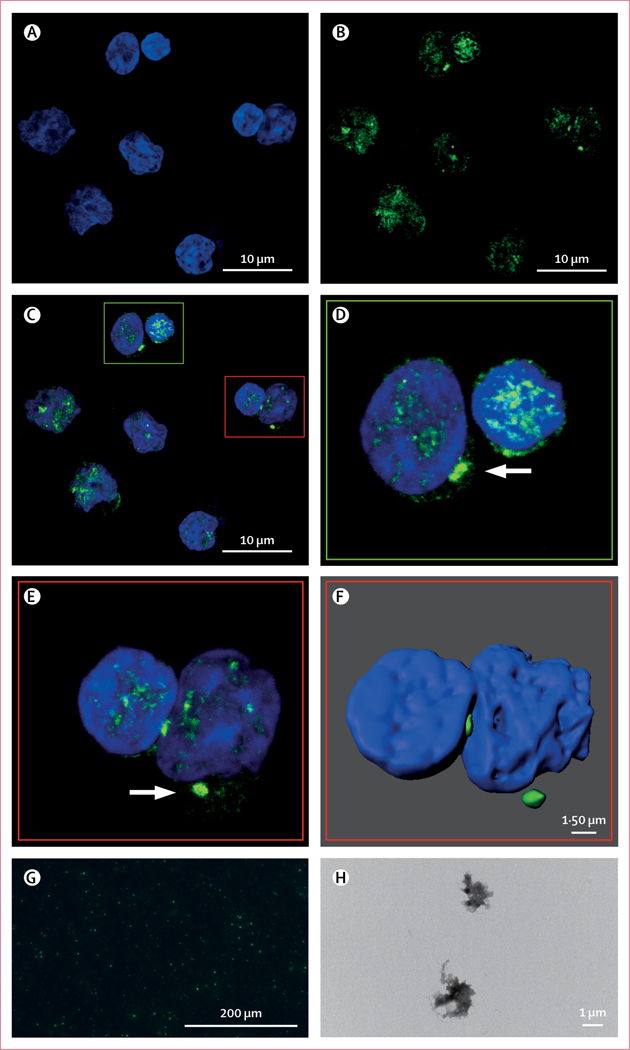
Background: NLRP3 inflammasome-directed pyroptotic cell death drives ineffective haemopoiesis in myelodysplastic syndromes. During inflammasome assembly, the apoptosis-associated speck-like protein containing a CARD (PYCARD, commonly known as ASC) adaptor protein polymerises into large, filamentous clusters termed ASC specks that are released upon cytolysis. Specks are resistant to proteolytic degradation because of their prion-like structure, and therefore might serve as a biomarker for pyroptotic cell death in myelodysplastic syndromes.
Methods: This observational cohort study was done at the H Lee Moffitt Cancer Center (Tampa, FL, USA). Patients with myelodysplastic syndromes, healthy controls, and patients with non-myelodysplastic syndrome haematological cancers or type 2 diabetes were recruited. We used confocal and electron microscopy to visualise, and flow cytometry to quantify, ASC specks in peripheral blood and bone marrow plasma samples. Speck percentages were compared by t test or ANOVA, correlations were assessed by Spearman's rank correlation coefficient, and biomarker efficiency was assessed by receiver operating characteristics and area under the curve (AUC) analysis.
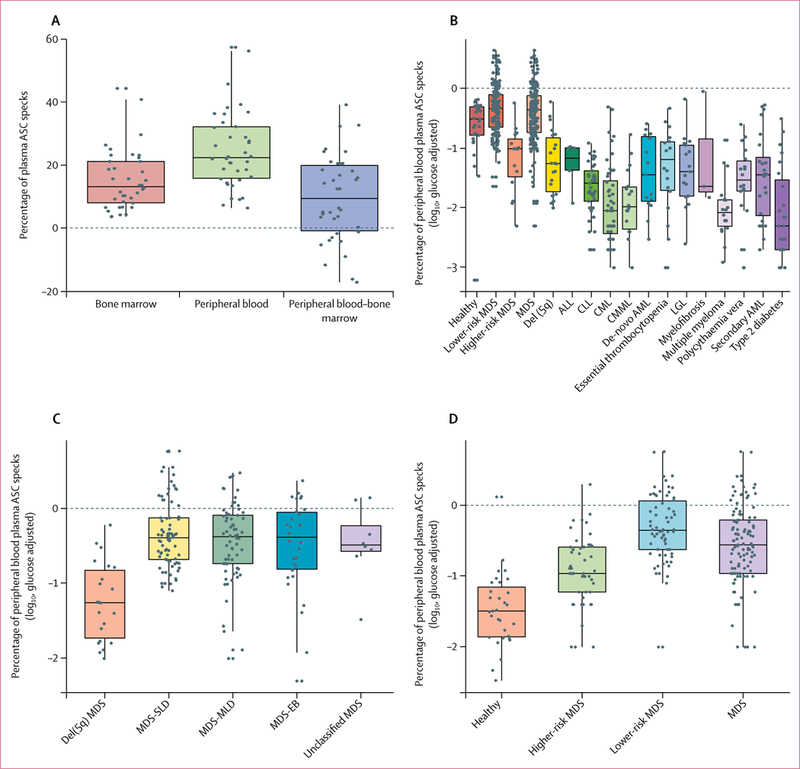
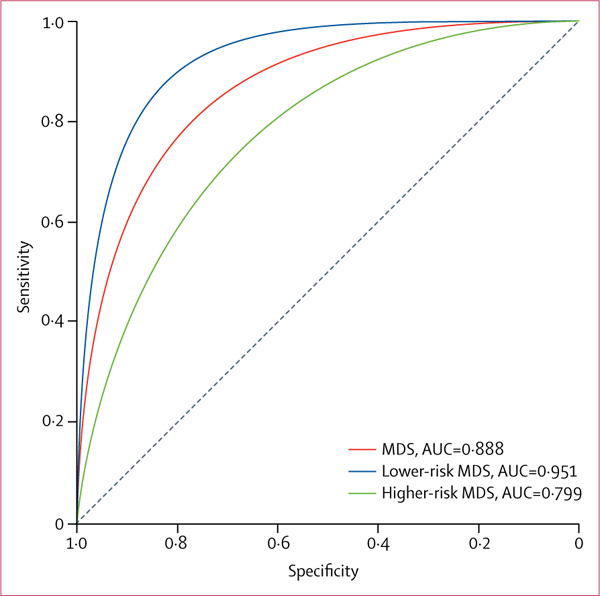
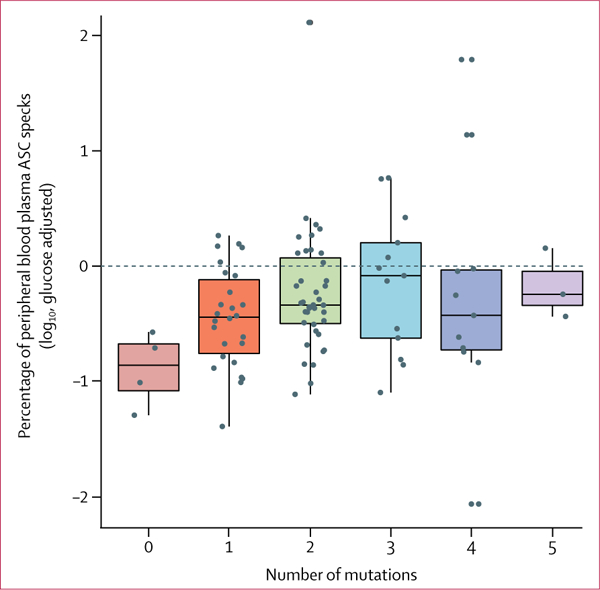
Findings: Between Jan 1, 2005, and Jan 12, 2017, we obtained samples from 177 patients with myelodysplastic syndromes and 29 healthy controls for the discovery cohort, and 113 patients with myelodysplastic syndromes and 31 healthy controls for the validation cohort. We also obtained samples from 22 patients with del(5q) myelodysplastic syndromes, 230 patients with non-myelodysplastic syndrome haematological cancers and 23 patients with type 2 diabetes. After adjustment for glucose concentration, the log10-transformed mean percentage of peripheral blood plasma-derived ASC specks was significantly higher in the 177 patients with myelodysplastic syndromes versus the 29 age-matched, healthy donors (-0·41 [SD 0·49] vs -0·67 [0·59], p=0·034). The percentages of ASC specks in samples from patients with myelodysplastic syndromes were significantly greater than those in samples from individuals with every other haematological cancer studied (all p<0·05) except myelofibrosis (p=0·19). The findings were confirmed in the independent validation cohort (p<0·0001). Peripheral blood plasma danger-associated molecular pattern protein S100-A8 and protein S100-A9 concentrations from 144 patients with myelodysplastic syndromes from the discovery cohort directly correlated with ASC speck percentage (r=0·4, p<0·0001 for S100-A8 and r=0·2, p=0·017 for S100-A9). Patients with at least two somatic gene mutations had a significantly greater mean percentage of peripheral blood plasma ASC specks than patients with one or no mutation (-0·22 [SD 0·63] vs -0·53 [0·44], p=0·008). The percentage of plasma ASC specks was a robust marker for pyroptosis in myelodysplastic syndromes (AUC=0·888), in which a cutoff of 0·80 maximised sensitivity at 0·84 (95% CI 0·65-0·91) and specificity at 0·87 (0·58-0·97).
Interpretation: Our results underscore the pathobiological relevance of ASC specks and suggest that ASC specks are a sensitive and specific candidate plasma biomarker that provides an index of medullary pyroptotic cell death and ineffective haemopoiesis in patients with myelodysplastic syndromes.
Funding: T32 Training Grant (NIH/NCI 5T32 CA115308-08), Edward P Evans Foundation, The Taub Foundation Grants Program, the Flow Cytometry, Analytic Microscopy, and Tissue Core Facilities at the H Lee Moffitt Cancer Center and Research Institute, a National Cancer Institute-designated Comprehensive Cancer Center (P30-CA076292).
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
ASC specks: a biomarker for myelodysplastic syndromes?Lancet Haematol. 2018 Sep;5(9):e379-e380. doi: 10.1016/S2352-3026(18)30113-3. Epub 2018 Jul 30. Lancet Haematol. 2018. PMID: 30072145 No abstract available.
References
-
- Broz P, Dixit VM. Inflammasomes: mechanism of assembly, regulation and signalling. Nat Rev Immunol 2016; 16: 407–20. - PubMed
-
- Font P, Loscertales J, Soto C, et al. Interobserver variance in myelodysplastic syndromes with less than 5% bone marrow blasts: unilineage vs. multilineage dysplasia and reproducibility of the threshold of 2% blasts. Ann Hematol 2015; 94: 565–73. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
