

BKV, CMV, and EBV Interactions and their Effect on Graft Function One Year Post-Renal Transplantation: Results from a Large Multi-Centre Study
- PMID: 30072213
- PMCID: PMC6116415
- DOI: 10.1016/j.ebiom.2018.07.017
BKV, CMV, and EBV Interactions and their Effect on Graft Function One Year Post-Renal Transplantation: Results from a Large Multi-Centre Study
Abstract
Background: BK virus (BKV), Cytomegalovirus (CMV) and Epstein-Barr virus (EBV) reactivations are common after kidney transplantation and associated with increased morbidity and mortality. Although CMV might be a risk factor for BKV and EBV, the effects of combined reactivations remain unknown. The purpose of this study is to ascertain the interaction and effects on graft function of these reactivations.
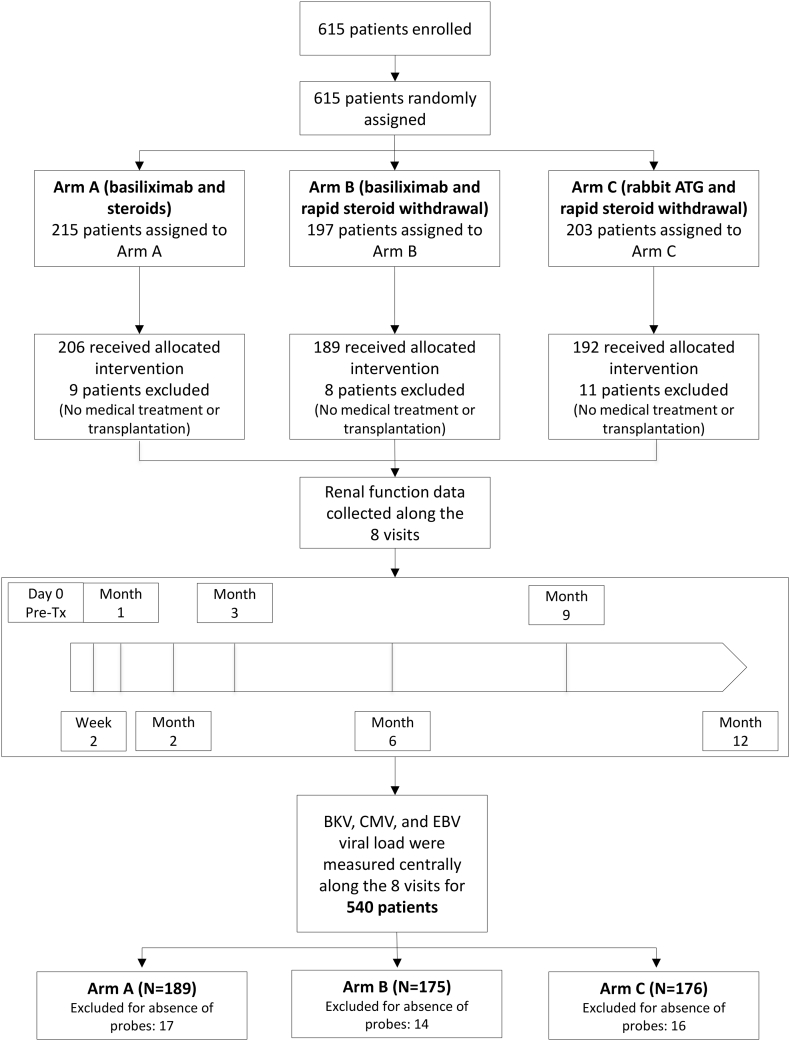
Methods: 3715 serum samples from 540 kidney transplant recipients were analysed for viral load by qPCR. Measurements were performed throughout eight visits during the first post-transplantation year. Clinical characteristics, including graft function (GFR), were collected in parallel.
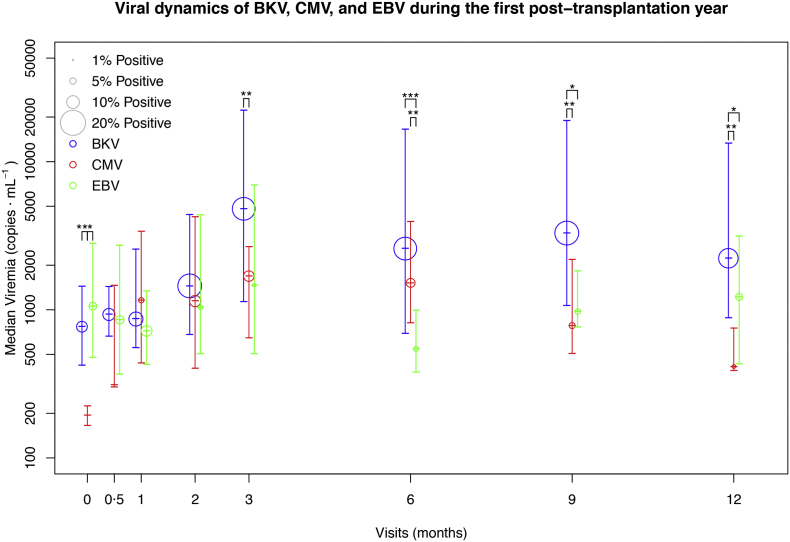
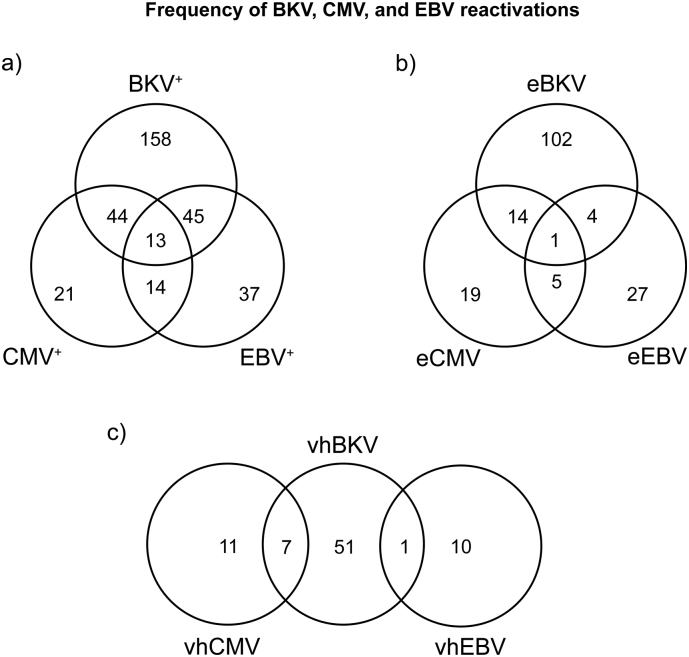
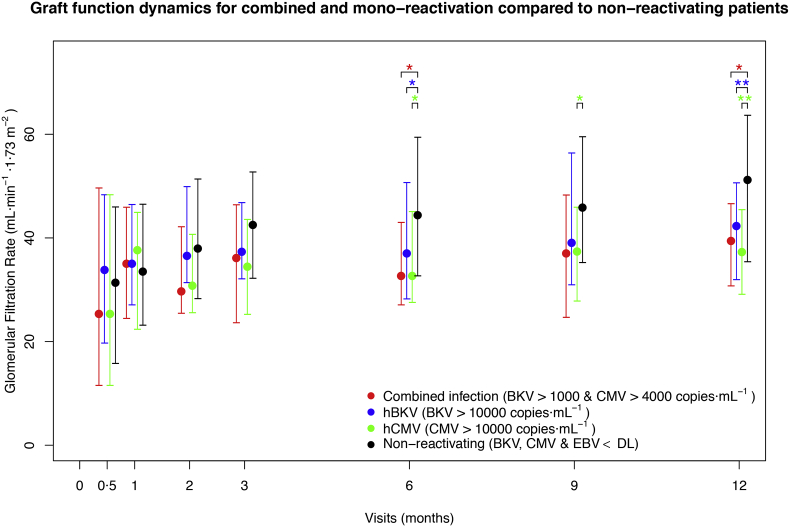
Findings: BKV had the highest prevalence and viral loads. BKV or CMV viral loads over 10,000 copies·mL-1 led to significant GFR impairment. 57 patients had BKV-CMV combined reactivation, both reactivations were significantly associated (p = 0.005). Combined reactivation was associated with a significant GFR reduction one year post-transplantation of 11.7 mL·min-1·1.73 m-2 (p = 0.02) at relatively low thresholds (BKV > 1000 and CMV > 4000 copies·mL-1). For EBV, a significant association was found with CMV reactivation (p = 0.02), but no GFR reduction was found. Long cold ischaemia times were a further risk factor for high CMV load.
Interpretation: BKV-CMV combined reactivation has a deep impact on renal function one year post-transplantation and therefore most likely on long-term allograft function, even at low viral loads. Frequent viral monitoring and subsequent interventions for low BKV and/or CMV viraemia levels and/or long cold ischaemia time are recommended. FUND: Investigator Initiated Trial; financial support by German Federal Ministry of Education and Research (BMBF).
Keywords: BK virus; Combined reactivation; Cytomegalovirus; Epstein-Barr virus; Graft function; Kidney transplantation.
Copyright © 2018 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Alangaden G.J., Rama T., Gruber S.A. Infectious complications after kidney transplantation: current epidemiology and associated risk factors. Clin Transplant. 2006;20:401–409. - PubMed
-
- Egli A., Infanti L., Dumoulin A. Prevalence of polyomavirus BK and JC infection and replication in 400 healthy blood donors. J Infect Dis. 2009;199:837–846. - PubMed
-
- Griffiths P., Baraniak I., Reeves M. The pathogenesis of human cytomegalovirus. J Pathol. 2015;235:288–297. - PubMed
-
- Ng S.-B., Khoury J.D. Epstein-Barr virus in lymphoproliferative processes: an update for the diagnostic pathologist. Adv Anat Pathol. 2009;16:40–55. - PubMed
-
- Le Page A.K., Mackie F.E., McTaggart S.J., Kennedy S.E. Cytomegalovirus & epstein barr virus serostatus as a predictor of the long-term outcome of kidney transplantation. Nephrology (Carlton) 2013;18:813–819. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
