

Evaluation of 11C-Methionine PET and Anatomic MRI Associations in Diffuse Intrinsic Pontine Glioma
- PMID: 30072503
- PMCID: PMC6424234
- DOI: 10.2967/jnumed.118.212514
Evaluation of 11C-Methionine PET and Anatomic MRI Associations in Diffuse Intrinsic Pontine Glioma
Abstract
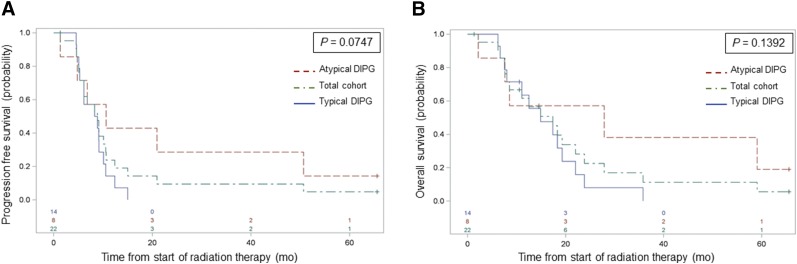
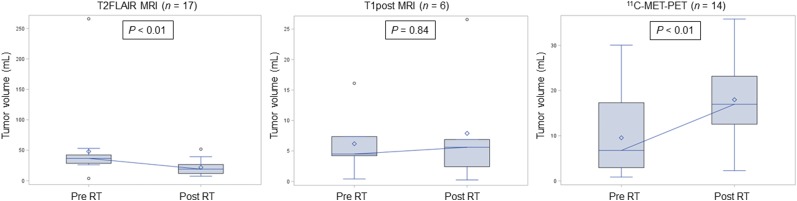
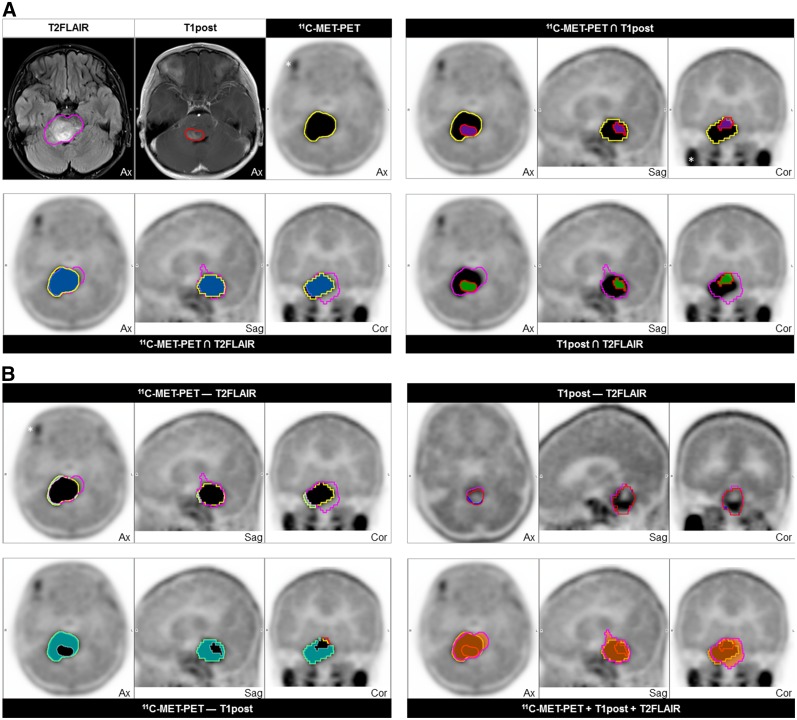
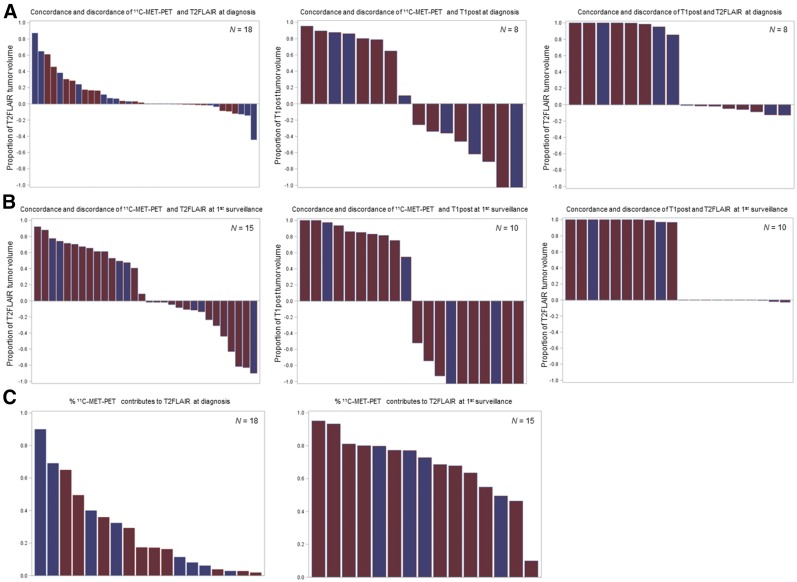
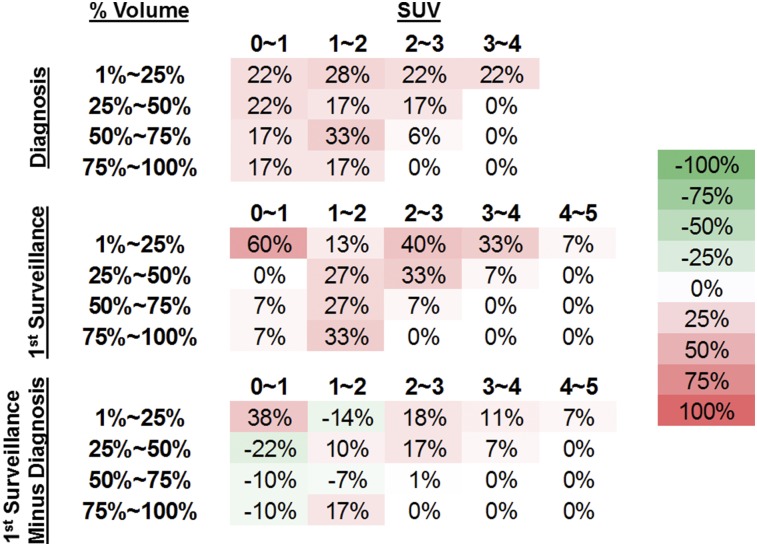
The role of metabolic imaging in the diagnosis, treatment, and response assessment of diffuse intrinsic pontine glioma (DIPG) is poorly defined. We investigated the uptake of 11C-methionine in pediatric patients with newly diagnosed DIPG and evaluated the associations of 11C-methionine PET metrics with conventional MRI indices and survival outcomes. Methods: Twenty-two patients with newly diagnosed DIPG were prospectively enrolled on an institutional review board-approved investigational study of 11C-methionine PET. All patients underwent baseline 11C-methionine PET/CT, and initial treatment-response scans after chemotherapy or radiation therapy were obtained for 17 patients. Typical and atypical DIPGs were assessed clinically and radiographically and defined by multidisciplinary consensus. Three-dimensional regions of interest, reviewed by consensus between a nuclear medicine physician and a radiation oncologist, were delineated after coregistration of PET and MR images. Associations of 11C-methionine uptake intensity and uniformity with survival, along with associations between 11C-methionine uptake and conventional MRI tumor indices over time, were evaluated. 11C-methionine PET voxel values within regions of interest were assessed as threshold values across proportions of the study population, and 11C-methionine uptake at baseline was assessed relative to MRI-defined tumor progression. Results:11C-methionine uptake above that of uninvolved brain tissue was observed in 18 of 22 baseline scans (82%) and 15 of 17 initial response scans (88%). 11C-methionine avidity within MRI-defined tumor was limited in extent, with 11 of 18 positive baseline 11C-methionine PET scans (61%) showing less than 25% 11C-methionine-avid tumor. The increase in total tumor volume with 11C-methionine PET was relatively limited (17.2%; interquartile range, 6.53%-38.90%), as was the extent of 11C-methionine uptake beyond the MRI-defined tumor (2.2%; interquartile range, 0.55%-10.88%). Although baseline 11C-methionine PET intensity and uniformity metrics did not correlate with survival outcomes, initial 11C-methionine avidity overlapped with recurrent tumor in 100% of cases. A clinical diagnosis of atypical DIPG was associated with borderline significantly prolonged progression-free survival (P = 0.07), yet 11C-methionine PET indices at diagnosis did not differ significantly between atypical and typical DIPGs. Conclusion: Most newly diagnosed DIPGs are successfully visualized by 11C-methionine PET. Baseline 11C-methionine uptake delineates regions at increased risk for recurrence, yet intensity and uniformity metrics did not correlate with treatment outcomes in children with DIPG in this study.
Keywords: 11C-methionine PET; DIPG; MRI; brainstem glioma; diffuse midline glioma; pediatric.
© 2019 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol (Berl). 2016;131:803–820. - PubMed
-
- Puget S, Beccaria K, Blauwblomme T, et al. Biopsy in a series of 130 pediatric diffuse intrinsic pontine gliomas. Childs Nerv Syst. 2015;31:1773–1780. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical