

The role of Neonatologist Performed Echocardiography in the assessment and management of neonatal shock
- PMID: 30072807
- PMCID: PMC6257224
- DOI: 10.1038/s41390-018-0081-1
The role of Neonatologist Performed Echocardiography in the assessment and management of neonatal shock
Abstract
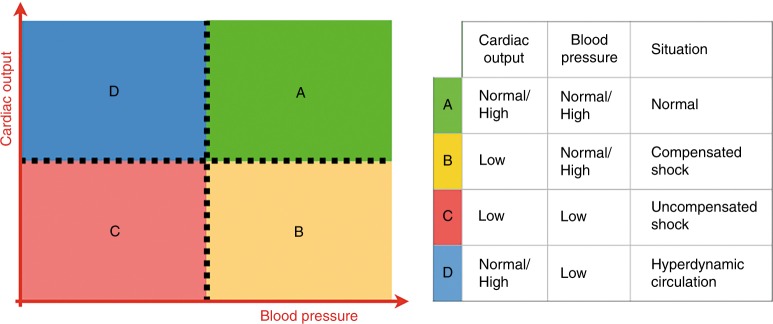
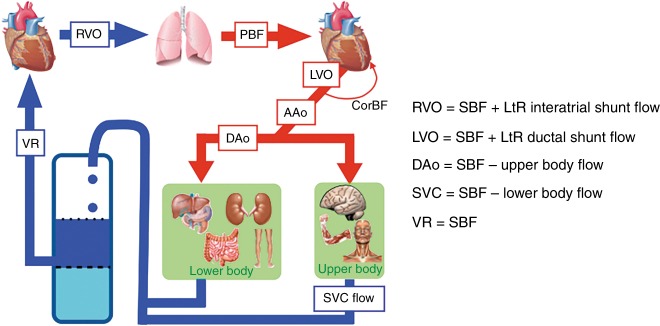
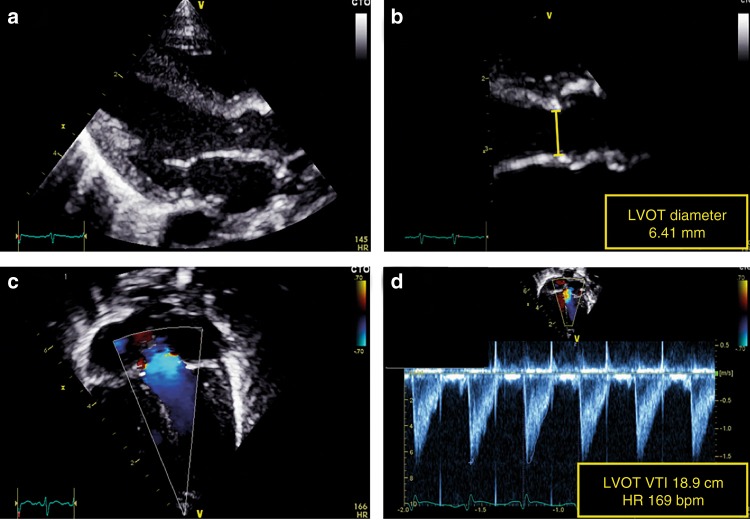
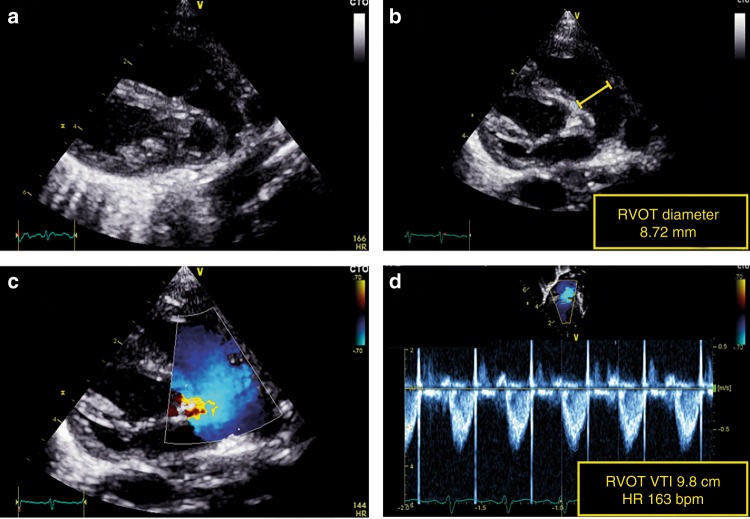
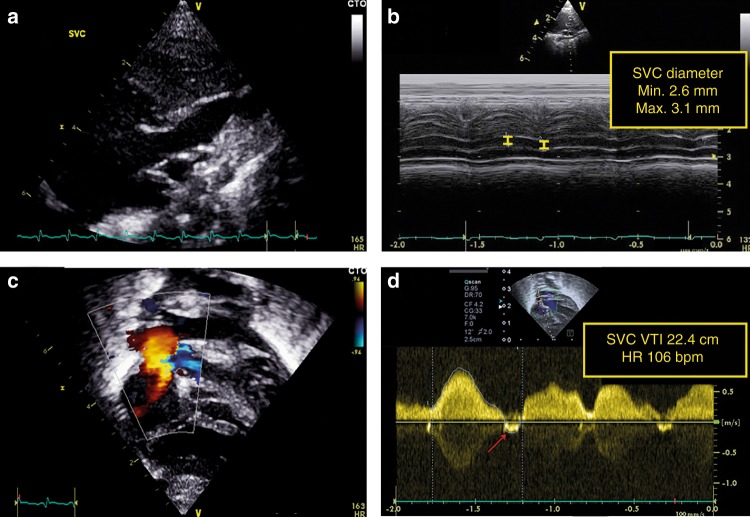
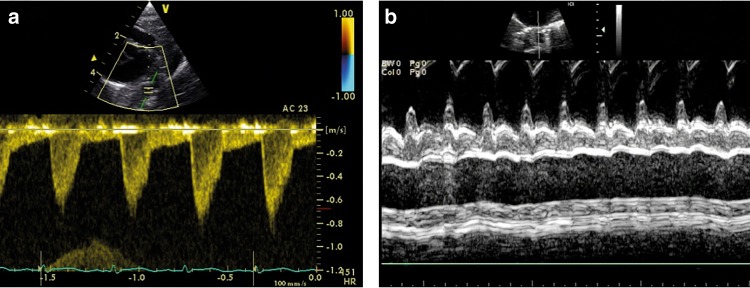
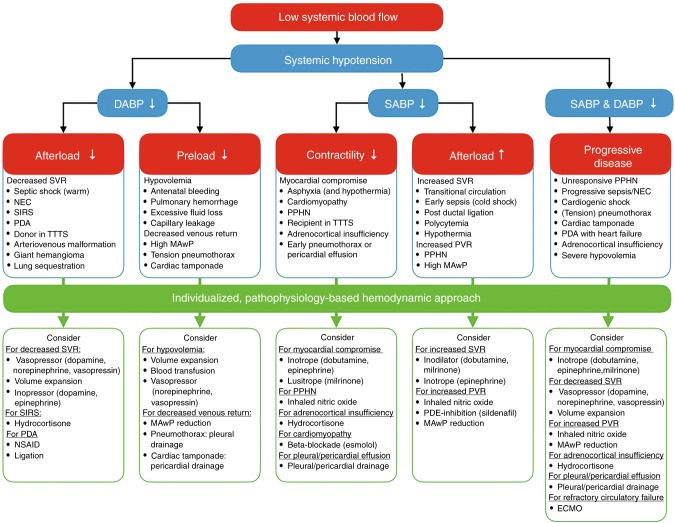
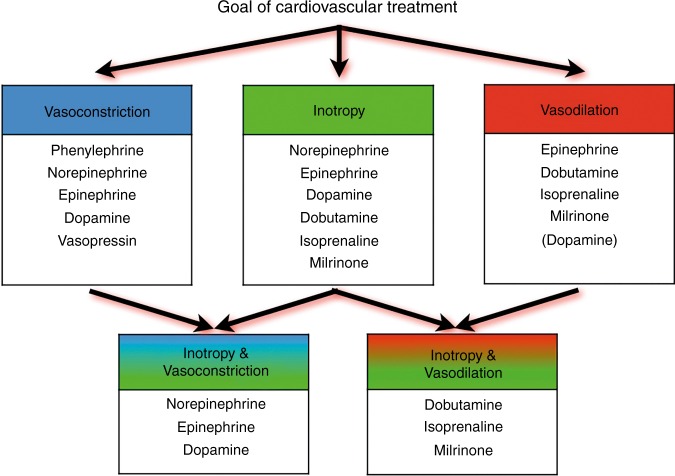
One of the major challenges of neonatal intensive care is the early detection and management of circulatory failure. Routine clinical assessment of the hemodynamic status of newborn infants is subjective and inaccurate, emphasizing the need for objective monitoring tools. An overview will be provided about the use of neonatologist-performed echocardiography (NPE) to assess cardiovascular compromise and guide hemodynamic management. Different techniques of central blood flow measurement, such as left and right ventricular output, superior vena cava flow, and descending aortic flow are reviewed focusing on methodology, validation, and available reference values. Recommendations are provided for individualized hemodynamic management guided by NPE.
Conflict of interest statement
A.E.-K. is in receipt of an Irish Health Research Board Clinical Trials Network Grant (HRB CTN 2014-10) and an EU FP7/2007-2013 grant (agreement no. 260777, The HIP Trial). A.M.G. owned equity in Neonatal Echo Skills and has received grant support from the American Heart Association. D.V.L. is in receipt of an EU FP7/2007-2013 (agreement no. 260777 the HIP trial). E.D. received lecture fees and consulting fees from Chiesi Pharmaceutical. E.N. received grant support from Research Council of Norway and Vestfold Hospital Trust. K.B. received lecture fees from Chiesi Pharmaceutical. M.B. holds a patent, “Thermal shield for the newborn baby. S.G. received grant support from National Institute of Health Research, Health Technology Assessment (11/92/15), UK. S.R.R. received lecture fees for Phillips Ultrasound and GE Ultrasound. W.P.B. has received grant support from The Netherlands Organization for Health and Development (ZonMw; grant numbers 843002622 and 843002608). Z.M. has received lecture fees from Chiesi Pharmaceutical. The other authors declare no competing interests.
Figures
Comment in
-
Targeted neonatal echocardiography in the United States of America: the contemporary perspective and challenges to implementation.Pediatr Res. 2019 Jun;85(7):919-921. doi: 10.1038/s41390-019-0338-3. Epub 2019 Feb 18. Pediatr Res. 2019. PMID: 30776791 No abstract available.
References
-
- Kleinman, C. S. & Seri, I. in Hemodynamics and Cardiology: Neonatology Questions and Controversies 2nd edn (ed. Polin, R. A.) (Elsevier Health Sciences, Amsterdam, 2012).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
