

Treatment of a Neglected Patellar Tendon Rupture with a Modified Surgical Technique: Ipsilateral Semitendinosus Autograft Reconstruction with Suture Tape Augmentation
- PMID: 30073104
- PMCID: PMC6057304
- DOI: 10.1155/2018/2037638
Treatment of a Neglected Patellar Tendon Rupture with a Modified Surgical Technique: Ipsilateral Semitendinosus Autograft Reconstruction with Suture Tape Augmentation
Abstract
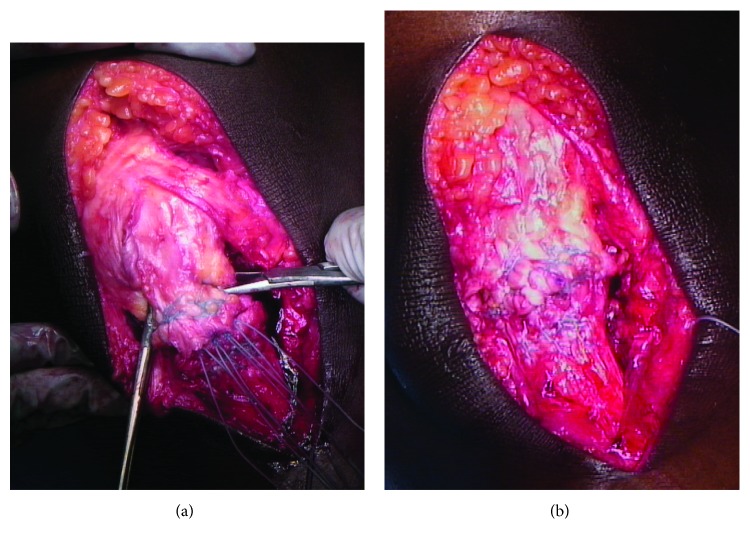
Patellar tendon ruptures are rare, but debilitating injuries are typically seen in young active males in the third and fourth decades of life. They can occur as a single acute injury or from repetitive microtrauma weakening the tendon. Patients typically present complaining of knee pain, swelling, and an inability to perform a straight leg raise. Most conventionally, these injuries are classified as acute (less than two weeks) or chronic (greater than two weeks) based upon the timing of presentation. In patients with patellar tendon ruptures and inability to perform a straight leg raise, patellar tendon repair is most often recommended. A subset of patients with chronic patellar tendon ruptures, however, presents several months after their initial injuries. These neglected patella tendon ruptures present a particularly challenging clinical scenario in which primary repair is often difficult or not possible. This case report describes a modification to an existing surgical technique for reconstructing the patellar tendon using an ipsilateral semitendinosus tendon autograft with suture tape augmentation.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
