

Efficacy and Safety of Further Lowering of Low-Density Lipoprotein Cholesterol in Patients Starting With Very Low Levels: A Meta-analysis
- PMID: 30073316
- PMCID: PMC6233651
- DOI: 10.1001/jamacardio.2018.2258
Efficacy and Safety of Further Lowering of Low-Density Lipoprotein Cholesterol in Patients Starting With Very Low Levels: A Meta-analysis
Abstract
Importance: In the Cholesterol Treatment Trialists Collaboration (CTTC), in patients starting with low-density lipoprotein cholesterol (LDL-C) levels of approximately 3.4 mmol/L (131.5 mg/dL), there was a 22% reduction in major vascular events per 1-mmol/L (38.7-mg/dL) lowering of LDL-C. The magnitude of clinical benefit of further LDL-C lowering in patients already with very low LDL-C levels remains debated.
Objective: To evaluate efficacy and safety of further lowering LDL-C levels in patient populations presenting with median LDL-C levels of 1.8 mmol/L (70 mg/dL) or less.
Data sources and study selection: The CTTC was used for statin data. For nonstatin therapy, Medline database was searched (2015-April 2018). Key inclusion criteria were a randomized, double-blind, controlled cardiovascular outcome trial of LDL-C lowering with data in populations starting with LDL-C levels averaging 1.8 mmol/L (70 mg/dL) or less.
Data extraction and synthesis: Two authors independently extracted data into standardized data sheets, and data were analyzed using meta-analysis.
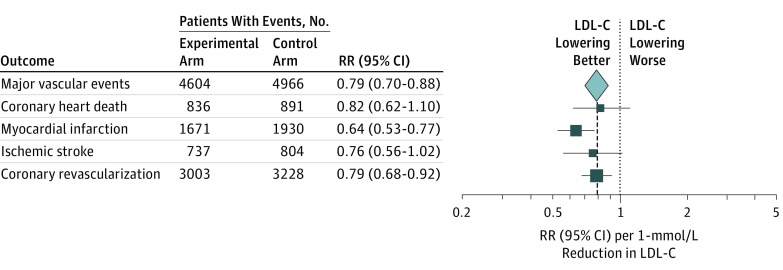
Main outcomes and measures: The risk ratio (RR) of major vascular events (a composite of coronary heart death, myocardial infarction, ischemic stroke, or coronary revascularization) per 1-mmol/L (38.7-mg/dL) reduction in LDL-C level.
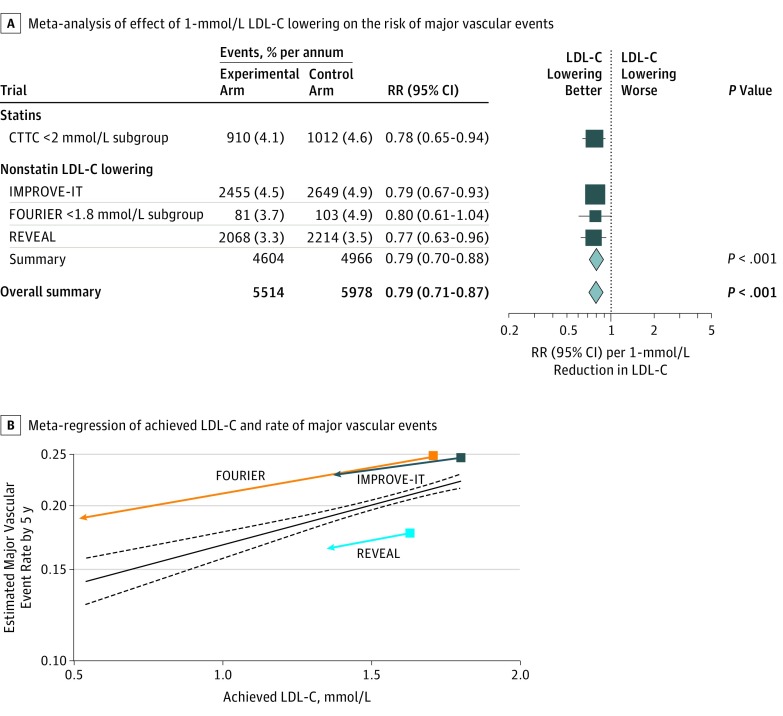
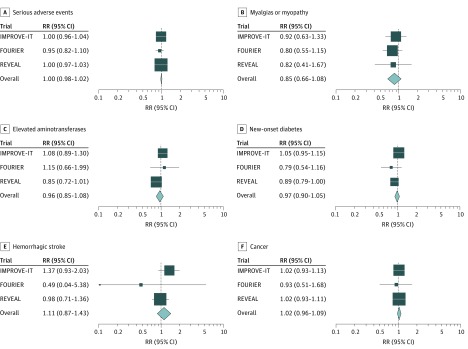
Results: In the subgroup of patients from the CTTC meta-analysis of statins with a mean LDL-C in the control arm of 1.7 mmol/L (65.7 mg/dL), 1922 major vascular events occurred and the RR for major vascular events per 1-mmol/L (38.7-mg/dL) reduction in LDL-C was 0.78 (95% CI, 0.65-0.94). For 3 trials of nonstatin LDL-C-lowering therapies added to statins, there were 50 627 patients, the median LDL-C in the control arms ranged from 1.6 mmol/L to 1.8 mmol/L (63 mg/dL to 70 mg/dL), and 9570 major vascular events occurred. Nonstatin therapy lowered LDL-C by 0.3 to 1.2 mmol/L (11 mg/dL to 45 mg/dL), and the RR for major vascular events per 1-mmol/L (38.7-mg/dL) reduction in LDL-C was 0.79 (95% CI, 0.70-0.88). For statins and nonstatins combined, the RR was 0.79 (95% CI, 0.71-0.87; P < .001). Low-density lipoprotein cholesterol lowering was not associated with an increased risk of serious adverse events, myalgias and/or myositis, elevation in the level of aminotransferases, new-onset diabetes, hemorrhagic stroke, or cancer.
Conclusions and relevance: There is a consistent relative risk reduction in major vascular events per change in LDL-C in patient populations starting as low as a median of 1.6 mmol/L (63 mg/dL) and achieving levels as low as a median of 0.5 mmol/L (21 mg/dL), with no observed offsetting adverse effects. These data suggest further lowering of LDL-C beyond the lowest current targets would further reduce cardiovascular risk.
Conflict of interest statement
Figures
Comment in
-
Low-Density Lipoprotein Cholesterol and Cardiovascular Risk Reduction: How Low Is Low Enough Without Causing Harm?JAMA Cardiol. 2018 Sep 1;3(9):802-803. doi: 10.1001/jamacardio.2018.2273. JAMA Cardiol. 2018. PMID: 30073330 No abstract available.
References
-
- Grundy SM, Cleeman JI, Merz CN, et al. ; National Heart, Lung, and Blood Institute; American College of Cardiology Foundation; American Heart Association . Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110(2):227-239. doi:10.1161/01.CIR.0000133317.49796.0E - DOI - PubMed
-
- Baigent C, Blackwell L, Emberson J, et al. ; Cholesterol Treatment Trialists’ (CTT) Collaboration . Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. doi:10.1016/S0140-6736(10)61350-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
