

Automation in intensity modulated radiotherapy treatment planning-a review of recent innovations
- PMID: 30074813
- PMCID: PMC6319857
- DOI: 10.1259/bjr.20180270
Automation in intensity modulated radiotherapy treatment planning-a review of recent innovations
Abstract
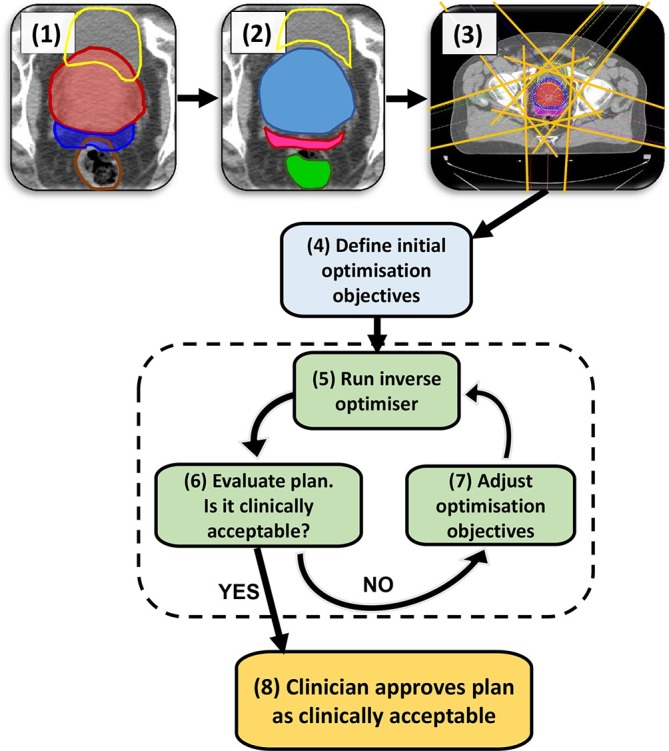
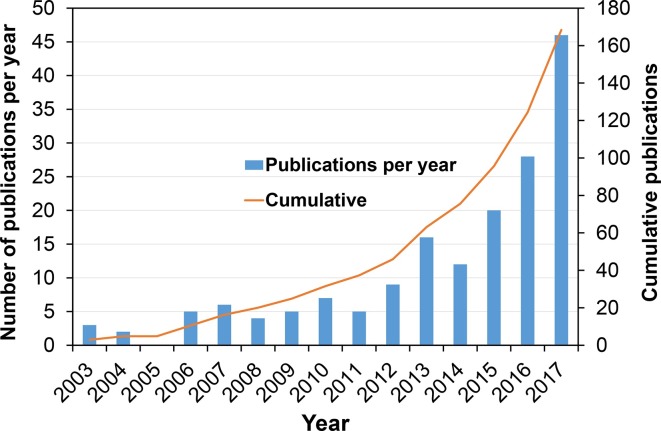
Radiotherapy treatment planning of complex radiotherapy techniques, such as intensity modulated radiotherapy and volumetric modulated arc therapy, is a resource-intensive process requiring a high level of treatment planner intervention to ensure high plan quality. This can lead to variability in the quality of treatment plans and the efficiency in which plans are produced, depending on the skills and experience of the operator and available planning time. Within the last few years, there has been significant progress in the research and development of intensity modulated radiotherapy treatment planning approaches with automation support, with most commercial manufacturers now offering some form of solution. There is a rapidly growing number of research articles published in the scientific literature on the topic. This paper critically reviews the body of publications up to April 2018. The review describes the different types of automation algorithms, including the advantages and current limitations. Also included is a discussion on the potential issues with routine clinical implementation of such software, and highlights areas for future research.
Figures
References
-
- Cancer Research, U. K, and NHS England . Vision for radiotherapy 2014-2024. London: Available at:https://www.cancerresearchuk.org/sites/default/files/policy_feb2014_radi... (Accessed 02/07/2018). 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
