

Cardiac CT in prosthetic aortic valve complications
- PMID: 30074821
- PMCID: PMC6435053
- DOI: 10.1259/bjr.20180237
Cardiac CT in prosthetic aortic valve complications
Abstract
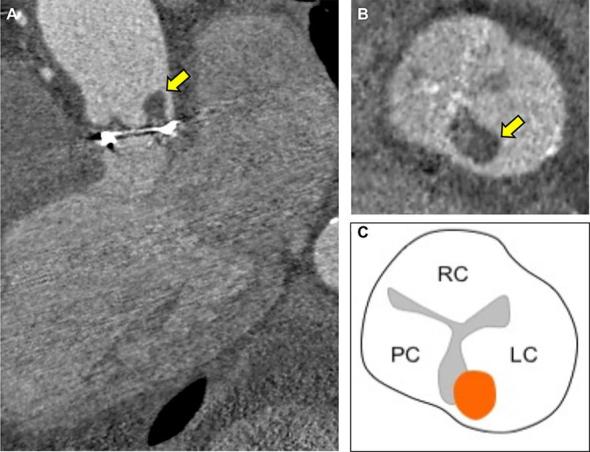
In the current era of transcatheter device therapy, the prevalence of prosthetic aortic valves and their associated complications is increasing. Echocardiography remains the first-line imaging investigation for the assessment of prosthetic valve complications, however, this often fails to identify the underlying mechanism of prosthesis failure. Recently, cardiac CT has emerged as an imaging technique capable of providing high isotropic spatial resolution of the prosthetic valve and its utility can provide important complementary diagnostic information. In this pictorial review, we present a series of common prosthetic aortic valve complications imaged with cardiac CT and demonstrate how use of this modality can enhance diagnostic accuracy.
Figures





References
-
- Grant SW, Hickey GL, Ludman P, Moat N, Cunningham D, de Belder M, et al. . Activity and outcomes for aortic valve implantations performed in England and Wales since the introduction of transcatheter aortic valve implantation. Eur J Cardiothorac Surg 2016; 49: 1164–73. doi: 10.1093/ejcts/ezv270 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
