

Left ventricular systolic function evaluated by strain echocardiography and relationship with mortality in patients with severe sepsis or septic shock: a systematic review and meta-analysis
- PMID: 30075792
- PMCID: PMC6091069
- DOI: 10.1186/s13054-018-2113-y
Left ventricular systolic function evaluated by strain echocardiography and relationship with mortality in patients with severe sepsis or septic shock: a systematic review and meta-analysis
Abstract
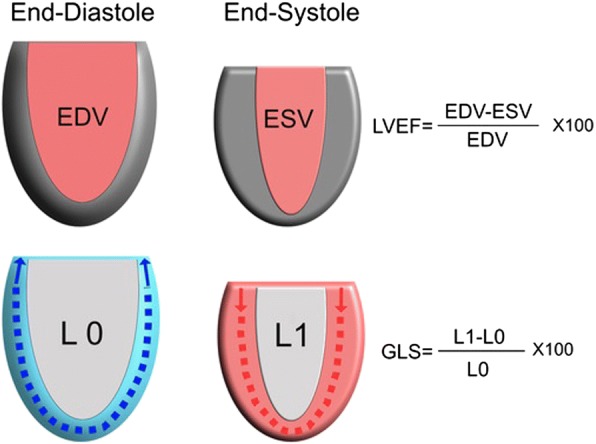
Background: Sepsis-induced myocardial dysfunction is associated with poor outcomes, but traditional measurements of systolic function such as left ventricular ejection fraction (LVEF) do not directly correlate with prognosis. Global longitudinal strain (GLS) utilizing speckle-tracking echocardiography (STE) could be a better marker of intrinsic left ventricular (LV) function, reflecting myocardial deformation rather than displacement and volume changes. We sought to investigate the prognostic value of GLS in patients with sepsis and/or septic shock.
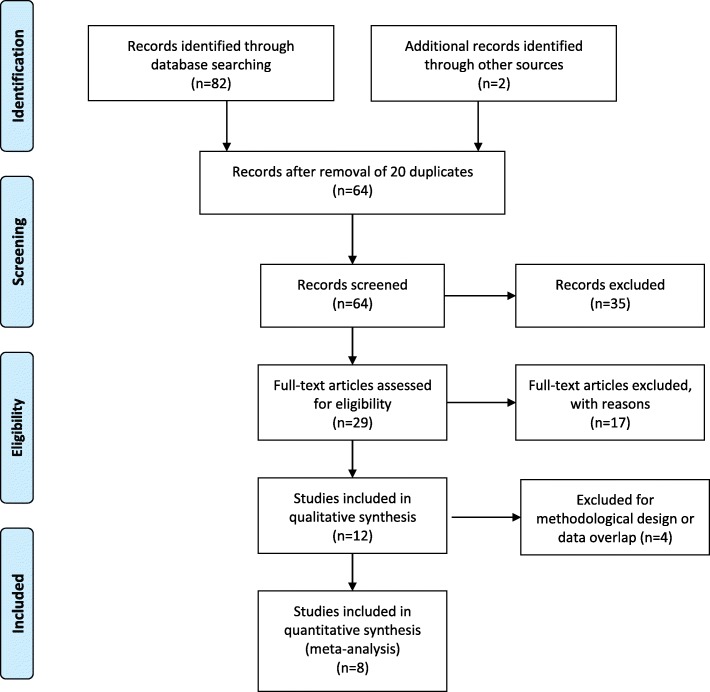
Methods: We conducted a systematic review (PubMed and Embase up to 26 October 2017) and meta-analysis to investigate the association between GLS and mortality at longest follow up in patients with severe sepsis and/or septic shock. In the primary analysis, we included studies reporting transthoracic echocardiography data on GLS according to mortality. A secondary analysis evaluated the association between LVEF and mortality including data from studies reporting GLS.
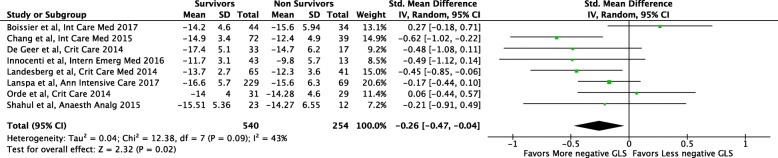
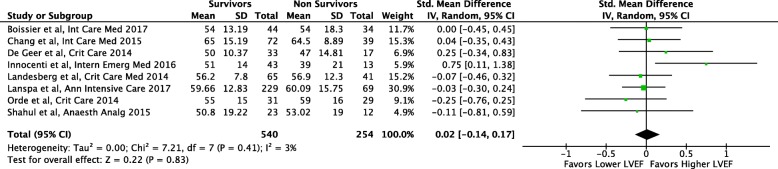
Results: We included eight studies in the primary analysis with a total of 794 patients (survival 68%, n = 540). We found a significant association between worse LV function and GLS values and mortality: standard mean difference (SMD) - 0.26; 95% confidence interval (CI) - 0.47, - 0.04; p = 0.02 (low heterogeneity, I2 = 43%). No significant association was found between LVEF and mortality in the same population of patients (eight studies; SMD, 0.02; 95% CI - 0.14, 0.17; p = 0.83; no heterogeneity, I2 = 3%).
Conclusions: Worse GLS (less negative) values are associated with higher mortality in patients with severe sepsis or septic shock, while such association is not valid for LVEF. More critical care research is warranted to confirm the better ability of STE in demonstrating underlying intrinsic myocardial disease compared to LVEF.
Keywords: Global longitudinal strain; Intensive care; Left ventricular ejection fraction; Speckle tracking; Systolic dysfunction.
Conflict of interest statement
Not applicable.
Not applicable.
The authors declare that they have no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Letter on "Left ventricular systolic function evaluated by strain echocardiography and relationship with mortality in patients with severe sepsis or septic shock: a systematic review and meta-analysis".Crit Care. 2019 Feb 8;23(1):38. doi: 10.1186/s13054-019-2312-1. Crit Care. 2019. PMID: 30736846 Free PMC article. No abstract available.
References
-
- Antonelli M, Bonten M, Chastre J, Citerio G, Conti G, Curtis JR, De Backer D, Hedenstierna G, Joannidis M, Macrae D, et al. Year in review in intensive care medicine 2011. II. Cardiovascular, infections, pneumonia and sepsis, critical care organization and outcome, education, ultrasonography, metabolism and coagulation. Intensive Care Med. 2012;38(3):345–358. doi: 10.1007/s00134-012-2467-6. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
