

Characteristics and outcomes of elderly patients with diffuse gliomas: a multi-institutional cohort study by Kansai Molecular Diagnosis Network for CNS Tumors
- PMID: 30076584
- PMCID: PMC6244782
- DOI: 10.1007/s11060-018-2957-7
Characteristics and outcomes of elderly patients with diffuse gliomas: a multi-institutional cohort study by Kansai Molecular Diagnosis Network for CNS Tumors
Abstract
Introduction: This study investigates the current state of clinical practice and molecular analysis for elderly patients with diffuse gliomas and aims to elucidate treatment outcomes and prognostic factors of patients with glioblastomas.
Methods: We collected elderly cases (≥ 70 years) diagnosed with primary diffuse gliomas and enrolled in Kansai Molecular Diagnosis Network for CNS Tumors. Clinical and pathological characteristics were analyzed retrospectively. Various factors were evaluated in univariate and multivariate models to examine their effects on overall survival.
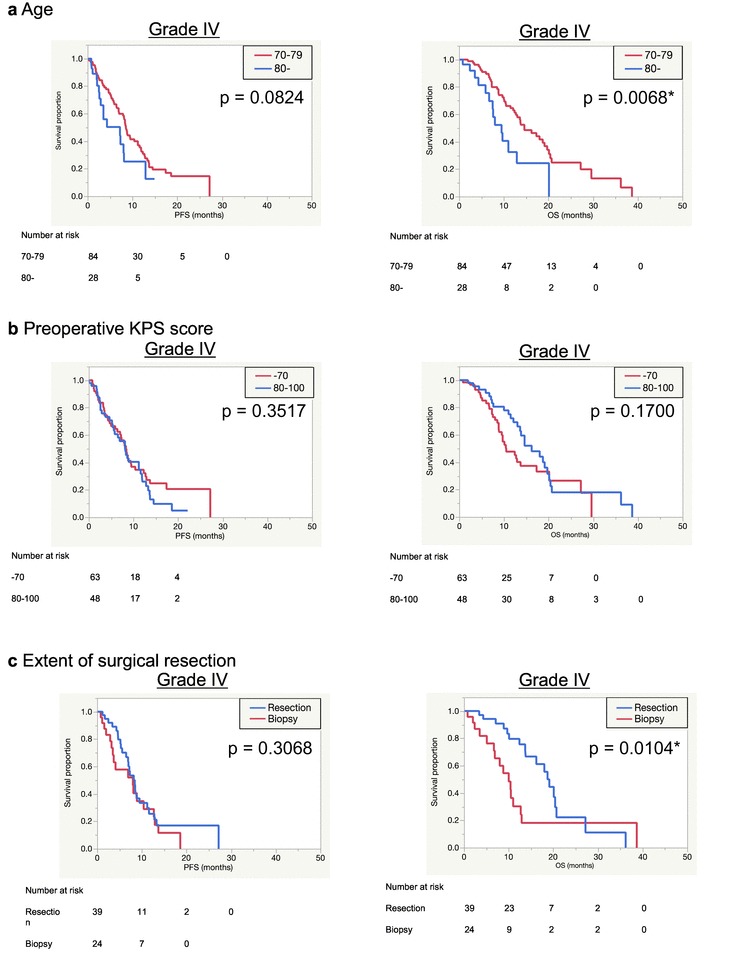
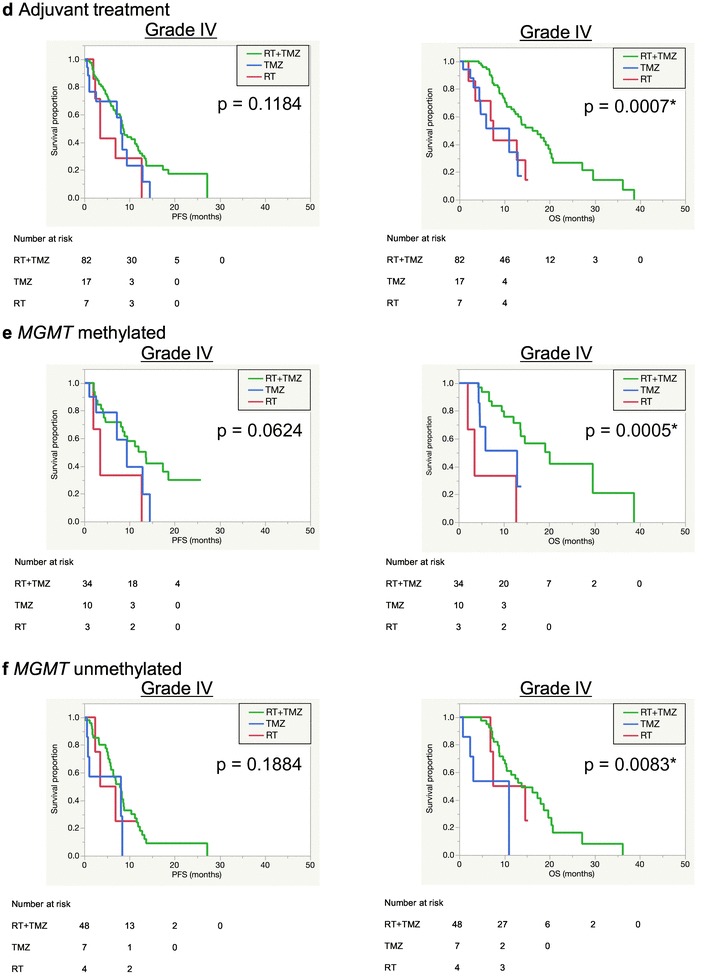
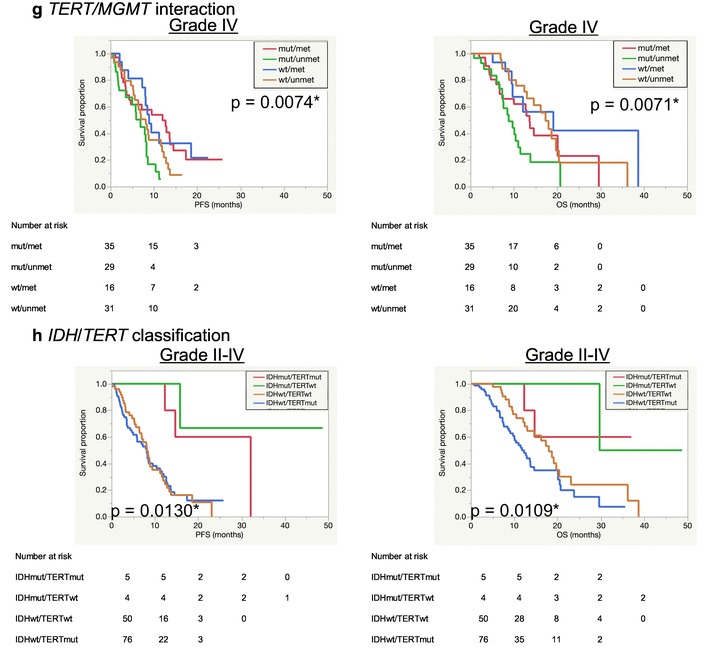
Results: Included in the study were 140 elderly patients (WHO grade II: 7, III: 19, IV: 114), median age was 75 years. Sixty-seven patients (47.9%) had preoperative Karnofsky Performance Status score of ≥ 80. All patients underwent resection (gross-total: 20.0%, subtotal: 14.3%, partial: 39.3%, biopsy: 26.4%). Ninety-six of the patients (68.6%) received adjuvant treatment consisting of radiotherapy (RT) with temozolomide (TMZ). Seventy-eight of the patients (75.0%) received radiation dose of ≥ 50 Gy. MGMT promoter was methylated in 68 tumors (48.6%), IDH1/2 was wild-type in 129 tumors (92.1%), and TERT promoter was mutated in 78 of 128 tumors (60.9%). Median progression-free and overall survival of grade IV cases was 8.2 and 13.6 months, respectively. Higher age (≥ 80 years) and TERT promoter mutated were associated with shorter survival. Resection and adjuvant RT + TMZ were identified as independent factors for good prognosis.
Conclusions: This community-based study reveals characteristics and outcomes of elderly glioma patients in a real-world setting. Elderly patients have several potential factors for poor prognosis, but resection followed by RT + TMZ could lengthen duration of survival.
Keywords: Diffuse glioma; Elderly; Glioblastoma; Molecular marker; Prognostic factor; Real-world data.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Committee of Brain Tumor Registry of Japan Report of Brain Tumor Registry of Japan (2001–2004) Neurol Med Chir (Tokyo) 2014;54(suppl.):1–102.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
