

Early treatment versus expectative management of patent ductus arteriosus in preterm infants: a multicentre, randomised, non-inferiority trial in Europe (BeNeDuctus trial)
- PMID: 30077184
- PMCID: PMC6090763
- DOI: 10.1186/s12887-018-1215-7
Early treatment versus expectative management of patent ductus arteriosus in preterm infants: a multicentre, randomised, non-inferiority trial in Europe (BeNeDuctus trial)
Abstract
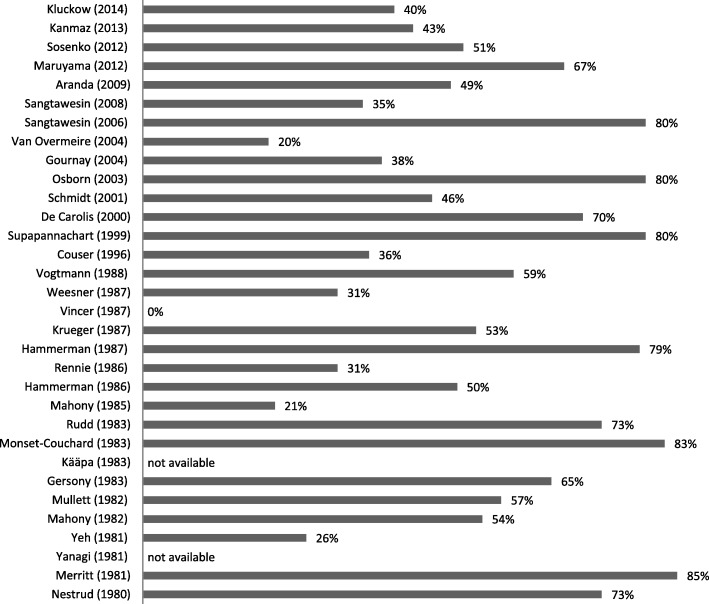
Background: Much controversy exists about the optimal management of a patent ductus arteriosus (PDA) in preterm infants, especially in those born at a gestational age (GA) less than 28 weeks. No causal relationship has been proven between a (haemodynamically significant) PDA and neonatal complications related to pulmonary hyperperfusion and/or systemic hypoperfusion. Although studies show conflicting results, a common understanding is that medical or surgical treatment of a PDA does not seem to reduce the risk of major neonatal morbidities and mortality. As the PDA might have closed spontaneously, treated children are potentially exposed to iatrogenic adverse effects. A conservative approach is gaining interest worldwide, although convincing evidence to support its use is lacking.
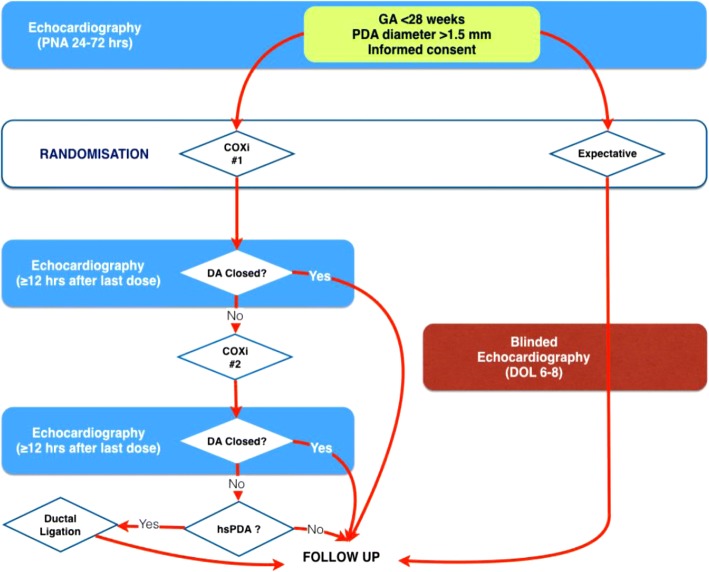
Methods: This multicentre, randomised, non-inferiority trial is conducted in neonatal intensive care units. The study population consists of preterm infants (GA < 28 weeks) with an echocardiographic-confirmed PDA with a transductal diameter > 1.5 mm. Early treatment (between 24 and 72 h postnatal age) with the cyclooxygenase inhibitor (COXi) ibuprofen (IBU) is compared with an expectative management (no intervention intended to close a PDA). The primary outcome is the composite of mortality, and/or necrotising enterocolitis (NEC) Bell stage ≥ IIa, and/or bronchopulmonary dysplasia (BPD) defined as the need for supplemental oxygen, all at a postmenstrual age (PMA) of 36 weeks. Secondary outcome parameters are short term sequelae of cardiovascular failure, comorbidity and adverse events assessed during hospitalization and long-term neurodevelopmental outcome assessed at a corrected age of 2 years. Consequences regarding health economics are evaluated by cost effectiveness analysis and budget impact analysis.
Discussion: As a conservative approach is gaining interest, we investigate whether in preterm infants, born at a GA less than 28 weeks, with a PDA an expectative management is non-inferior to early treatment with IBU regarding to the composite outcome of mortality and/or NEC and/or BPD at a PMA of 36 weeks.
Trial registration: This trial is registered with the Dutch Trial Register NTR5479 (registered on 19 October 2015), the registry sponsored by the United States National Library of Medicine Clinicaltrials.gov NCT02884219 (registered May 2016) and the European Clinical Trials Database EudraCT 2017-001376-28 .
Keywords: Bronchopulmonary dysplasia; Cost-effectiveness; Ductal ligation; Expectative management; Ibuprofen; Mortality; Necrotising enterocolitis; Neonatal intensive care unit; Patent ductus arteriosus; Prematurity.
Conflict of interest statement
This study has been approved by the MEC of the Radboud University (CMO Arnhem-Nijmegen; Number 2016–2552/NL57885.091.16). Neonates are only included after written informed consent is obtained from their parents or caregivers.
Not applicable.
The authors declare that they have no competing interests.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
