

C3 Glomerulopathy: Ten Years' Experience at Mayo Clinic
- PMID: 30077216
- PMCID: PMC6312642
- DOI: 10.1016/j.mayocp.2018.05.019
C3 Glomerulopathy: Ten Years' Experience at Mayo Clinic
Abstract
Objective: To describe the clinicopathological features, complement abnormalities, triggers, treatment, and outcomes of C3 glomerulopathy.
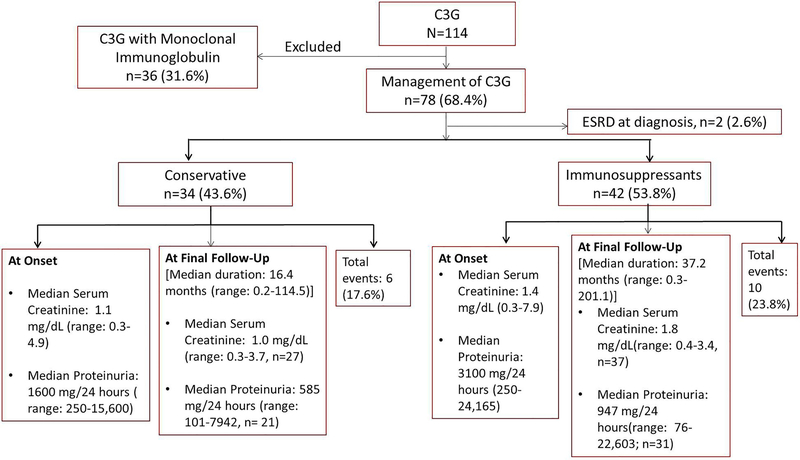
Patients and methods: A total of 114 patients with C3 glomerulopathy seen at Mayo Clinic from January 1, 2007, through December 31, 2016, were evaluated in this study.
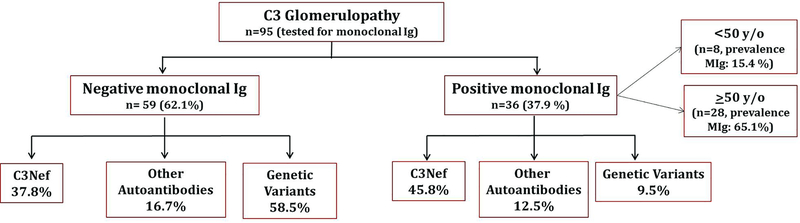
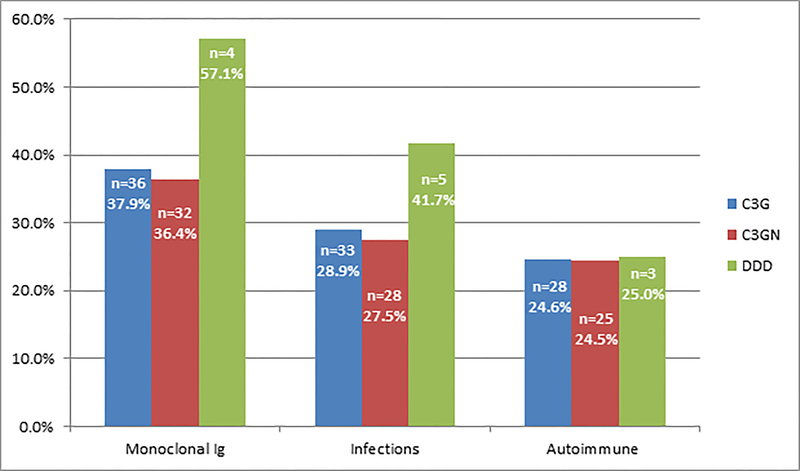
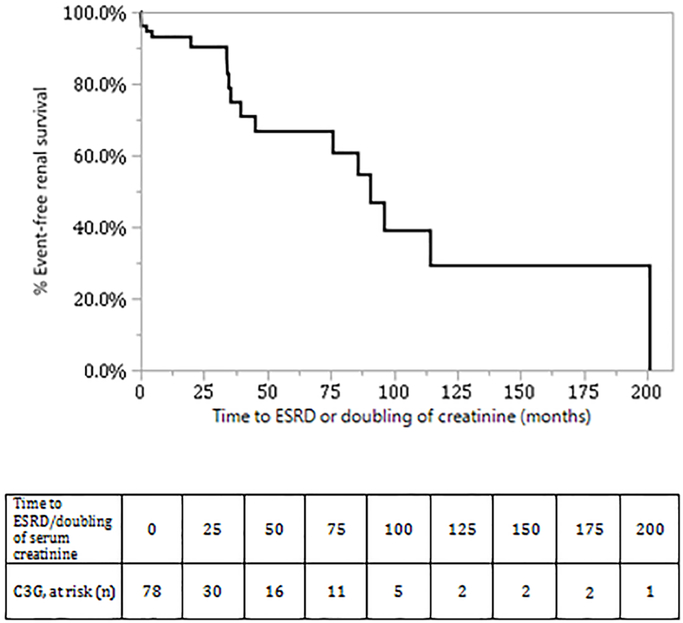
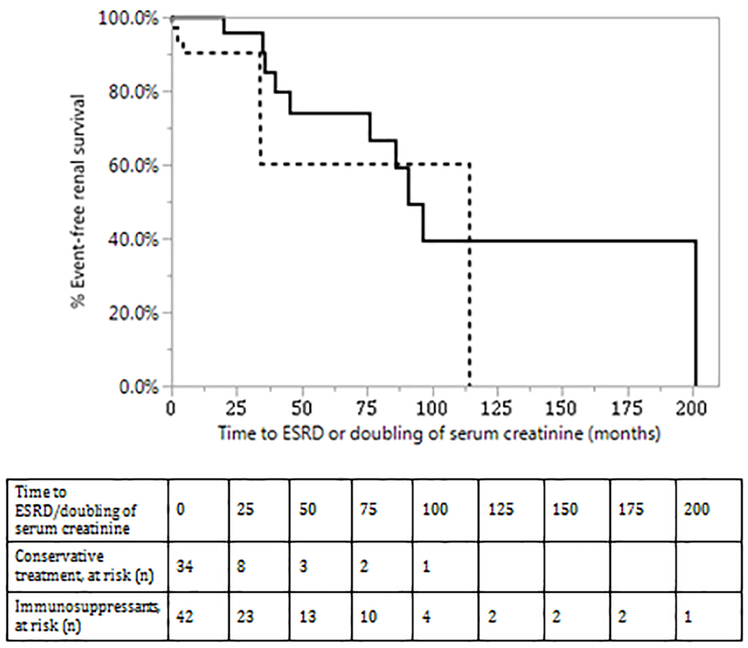
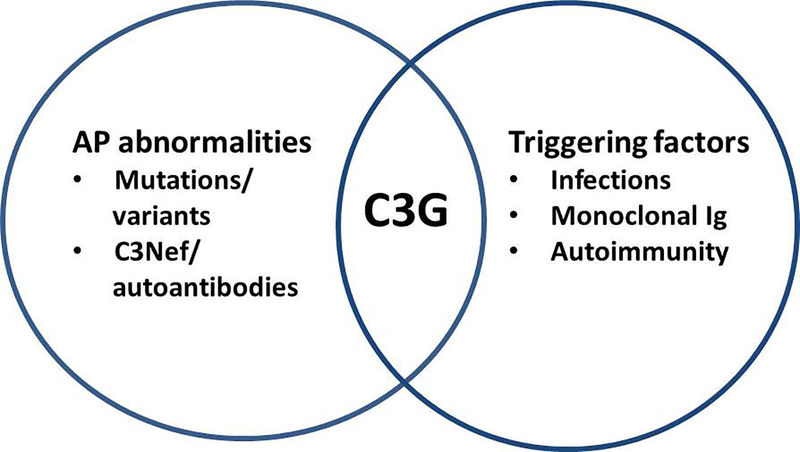
Results: The mean age at diagnosis for the entire cohort was 40.4±22.3 years, with a median serum creatinine level and proteinuria value of 1.6 mg/dL (range: 0.3-14.7) (to convert to mmol/L, multiply by 0.0259) and 2605 mg/24 h (range: 233-24,165), respectively. Hematuria was present in 100 patients (87.7%). The C3 and C4 levels were low in 50 of 112 (44.6%) and 13 of 110 (11.8%) patients, respectively. A history of infection, positive autoimmune findings, and monoclonal gammopathy (MIg) were present in 33 of 114 (28.9%), 28 of 114 (24.6%), and 36 of 95 (37.9%) patients, respectively. However, 28 of 43 patients 50 years or older (65.1%) had MIg. A genetic variant in complement genes, C3 nephritic factor (C3Nef), and other autoantibodies was present in 26 of 70 (37.1%), 30 of 69 (43.5%), and 9 of 67 (13.4%) patients, respectively. Membranoproliferative and mesangial proliferative glomerulonephritis were the common patterns of injury. Patients without MIg were younger (mean age, 32.3±20.6 years), with a median serum creatinine level and proteinuria value of 1.4 mg/dL (range: 0.3-7.9) and 2450 mg/24 h (range: 250-24, 165) and with low C3 and C4 levels in 38 of 77 (49.4%) and 9 of 75 (12.0%) patients, respectively. Most patients received corticosteroids and other immunosuppressive drugs. In patients without MIg, at a median follow-up of 22.3 months (range: 0.1-201.1), the median serum creatinine level and proteinuria value were 1.4 mg/dL (range: 0.3-3.7) and 825.5 mg/24 h (range: 76-22, 603), and 7 patients (9.2%) had progression to end-stage renal disease.
Conclusion: C3 glomerulopathy is a heterogeneous disease entity with complex triggering events and abnormalities of the alternative pathway of complement. The disease tends to be progressive and exhibits a variable response to immunosuppressive therapy.
Copyright © 2018 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: None
Figures
Comment in
-
C3 Glomerulopathy: A New Disease Comes of Age.Mayo Clin Proc. 2018 Aug;93(8):968-969. doi: 10.1016/j.mayocp.2018.06.014. Mayo Clin Proc. 2018. PMID: 30077212 No abstract available.
References
-
- Angioi A, Fervenza FC, Sethi S, et al. Diagnosis of complement alternative pathway disorders. Kidney International. 2016;89(2):278–288. - PubMed
-
- Servais A, Noel L- H, Roumenina LT, et al. Acquired and genetic complement abnormalities play a critical role in dense deposit disease and other C3 glomerulopathies. Kidney Int. 2012;82(4):454–464. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
