

Identification of beta-arrestin-1 as a diagnostic biomarker in lung cancer
- PMID: 30078843
- PMCID: PMC6162208
- DOI: 10.1038/s41416-018-0200-0
Identification of beta-arrestin-1 as a diagnostic biomarker in lung cancer
Abstract
Background: Distinguishing lung adenocarcinoma (ADC) from squamous cell carcinoma (SCC) has a tremendous therapeutic implication. Sometimes, the commonly used immunohistochemistry (IHC) markers fail to discriminate between them, urging for the identification of new diagnostic biomarkers.
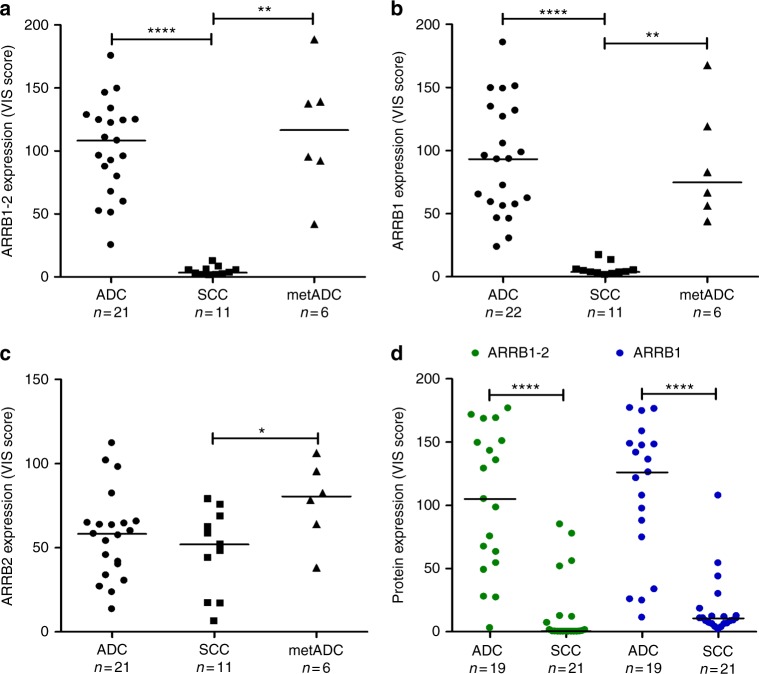
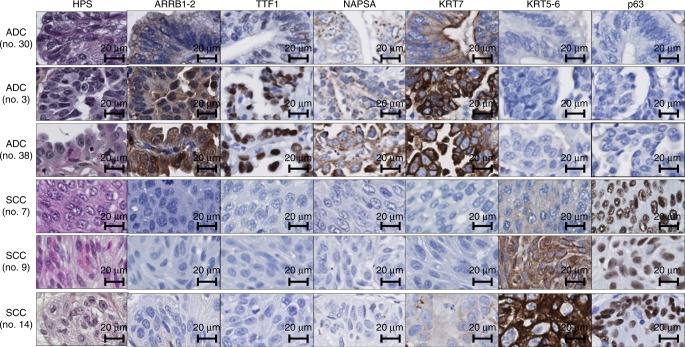
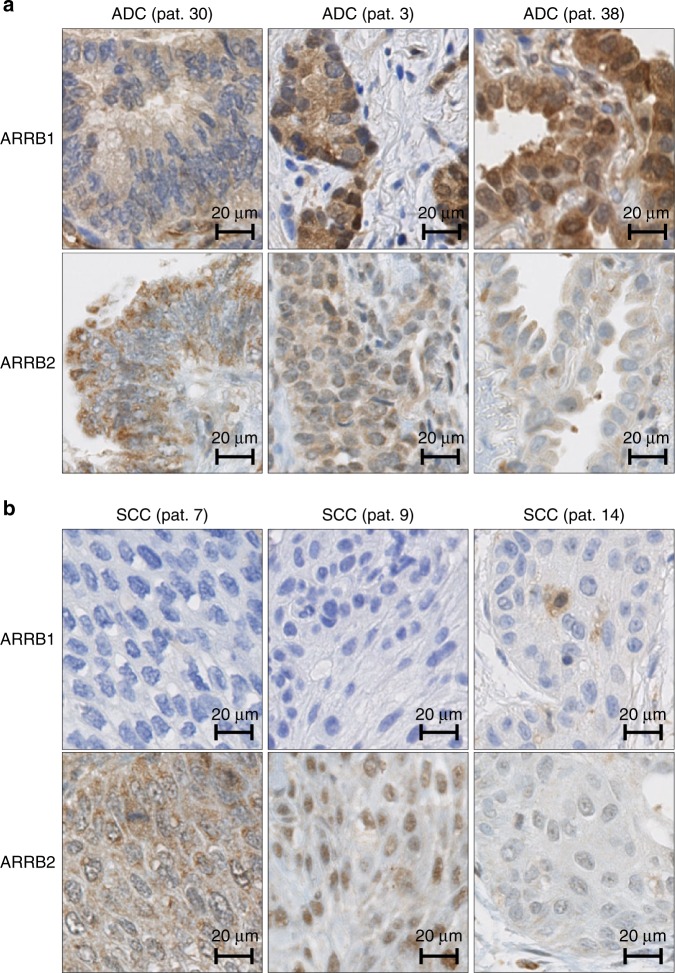
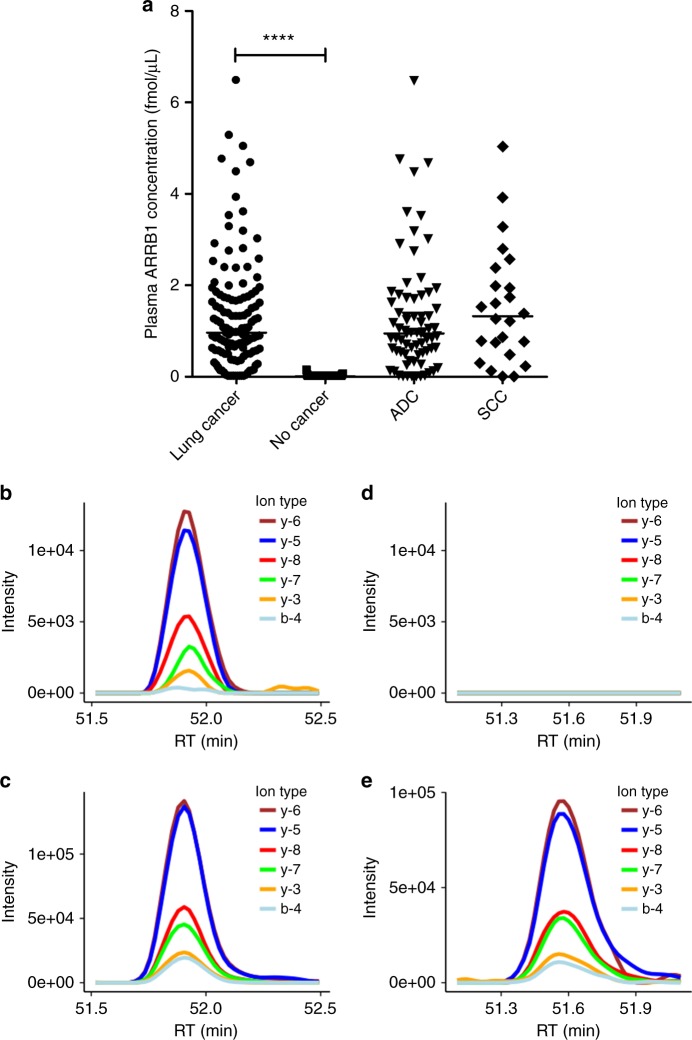
Methods: We performed IHC on tissue microarrays from two cohorts of lung cancer patients to analyse the expression of beta-arrestin-1, beta-arrestin-2 and clinically used diagnostic markers in ADC and SCC samples. Logistic regression models were applied for tumour subtype prediction. Parallel reaction monitoring (PRM)-based mass spectrometry was used to quantify beta-arrestin-1 in plasma from cancer patients and healthy donors.
Results: Beta-arrestin-1 expression was significantly higher in ADC versus SCC samples. Beta-arrestin-1 displayed high sensitivity, specificity and negative predictive value. Its usefulness in an IHC panel was also shown. Plasma beta-arrestin-1 levels were considerably higher in lung cancer patients than in healthy donors and were higher in patients who later experienced a progressive disease than in patients showing complete/partial response following EGFR inhibitor therapy.
Conclusions: Our data identify beta-arrestin-1 as a diagnostic marker to differentiate ADC from SCC and indicate its potential as a plasma biomarker for non-invasive diagnosis of lung cancer. Its utility to predict response to EGFR inhibitors is yet to be confirmed.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
