

Hepatectomy for gallbladder-cancer with unclassified anomaly of right-sided ligamentum teres: A case report and review of the literature
- PMID: 30079139
- PMCID: PMC6068848
- DOI: 10.4254/wjh.v10.i7.523
Hepatectomy for gallbladder-cancer with unclassified anomaly of right-sided ligamentum teres: A case report and review of the literature
Abstract
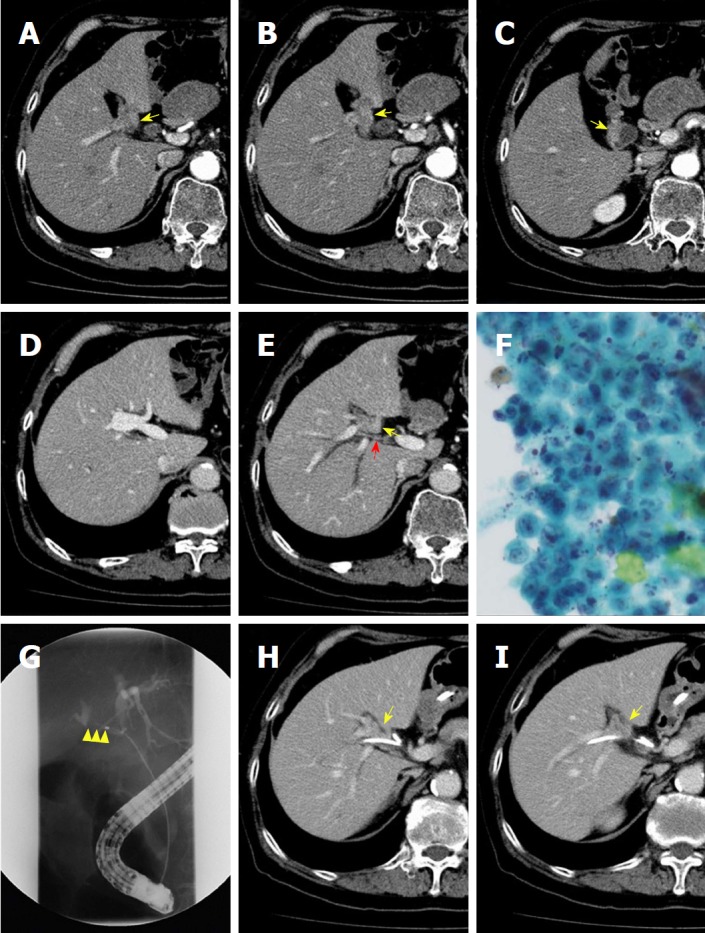
Right-sided ligamentum teres (RSLT) is a congenital anomaly in which the right umbilical ligament becomes dominant and anomalous ramifications of the hepatic vessels and biliary system are present. A male patient in his 70s was diagnosed with advanced gallbladder cancer directly infiltrating the right hepatic duct (RHD), together with RSLT. Preoperative three-dimensional simulation of the liver based on multiple detector computed tomography images after cholangiography revealed ramifications of all segmental portal veins from the portal trunk and discordance of the arterial and biliary branching patterns of segment 8. Fusion analysis of the biliary architecture and segmental volumetry showed that the RHD drained segments 1r, 5, 6, and 7. We successfully performed a modified right-sided hepatectomy sparing segment 8 (i.e., resection of the RHD drainage territory), with negative surgical margins. This report is the first to describe major hepatectomy for advanced gallbladder cancer with RSLT.
Keywords: Anomaly of the portal vein; Gallbladder cancer; Hepatectomy; Preoperative liver simulation; Right-sided ligamentum teres.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that no conflicts of interest are associated with this manuscript.
Figures







References
-
- Maetani Y, Itoh K, Kojima N, Tabuchi T, Shibata T, Asonuma K, Tanaka K, Konishi J. Portal vein anomaly associated with deviation of the ligamentum teres to the right and malposition of the gallbladder. Radiology. 1998;207:723–728. - PubMed
-
- Kawai K, Koizumi M, Honma S, Tokiyoshi A, Kodama K. Right ligamentum teres joining to the right branch of the portal vein. Anat Sci Int. 2008;83:49–54. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
