

Impact of incremental circumferential resection margin distance on overall survival and recurrence in oesophageal adenocarcinoma
- PMID: 30079392
- PMCID: PMC6069345
- DOI: 10.1002/bjs5.65
Impact of incremental circumferential resection margin distance on overall survival and recurrence in oesophageal adenocarcinoma
Abstract
Background: Previous analyses of the oesophageal circumferential resection margin (CRM) have focused on the prognostic validity of two different definitions of a positive CRM, that of the College of American Pathologists (tumour at margin) and that of the Royal College of Pathologists (tumour within 1 mm). This study aimed to analyse the validity of these definitions and explore the risk of recurrence and survival with incremental tumour distances from the CRM.
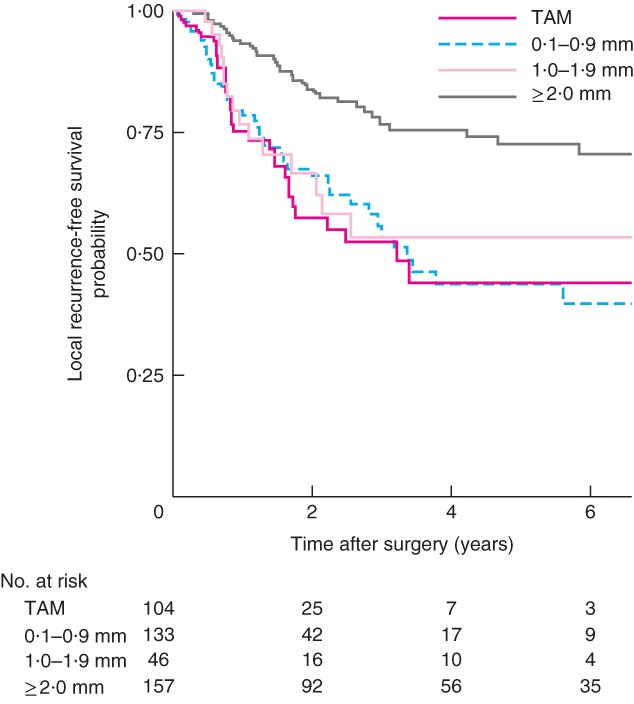
Methods: This cohort study included patients who underwent resection for adenocarcinoma of the oesophagus between 2000 and 2014. Kaplan-Meier and Cox regression analyses were performed to determine the hazard ratio (HR) with 95 per cent confidence intervals for recurrence and mortality in CRM increments: tumour at the cut margin, extending to within 0·1-0·9, 1·0-1·9, 2·0-4·9 mm, and 5·0 mm or more from the margin.
Results: A total of 444 patients were included in the study. Kaplan-Meier and unadjusted analyses showed a significant incremental improvement in overall survival (P < 0·001) and recurrence (P for trend < 0·001) rates with increasing distance from the CRM. Tumour distance of 2·0 mm or more remained a significant predictor of survival on multivariable analysis (HR for risk of death 0·66, 95 per cent c.i. 0·44 to 1·00). Multivariable analysis of overall survival demonstrated a significant difference between a positive and negative CRM with the Royal College of Pathologists' definition (HR 1·37, 1·01 to 1·85), but not with the College of American Pathologists' definition (HR 1·22, 0·90 to 1·65).
Conclusion: This study demonstrated an incremental improvement in survival and recurrence rates with increasing tumour distance from the CRM.
Figures




References
-
- Allum WH, Stenning SP, Bancewicz J, Clark PI, Langley RE. Long‐term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol 2009; 27: 5062–5067. - PubMed
-
- van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP et al; CROSS group. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med 2012; 366: 2074–2084. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M et al Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 2006: 355: 11–20. - PubMed
-
- Deeter M, Dorer R, Kuppusamy MK, Koehler RP, Low DE. Assessment of criteria and clinical significance of circumferential resection margins in esophageal cancer. Arch Surg 2009; 144: 618–624. - PubMed
-
- Harvin JA, Lahat G, Correa AM, Lee J, Maru D, Ajani J et al Neoadjuvant chemoradiotherapy followed by surgery for esophageal adenocarcinoma: significance of microscopically positive circumferential radial margins. J Thorac Cardiovasc Surg 2012; 143: 412–420. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
