

Longitudinal Phenotypes of Respiratory Health in a High-Risk Urban Birth Cohort
- PMID: 30079758
- PMCID: PMC6353010
- DOI: 10.1164/rccm.201801-0190OC
Longitudinal Phenotypes of Respiratory Health in a High-Risk Urban Birth Cohort
Abstract
Rationale: Characterization of patterns of wheezing and allergic sensitization in early life may allow for identification of specific environmental exposures impacting asthma development.
Objectives: To define respiratory phenotypes in inner-city children and their associations with early-life environmental exposures.
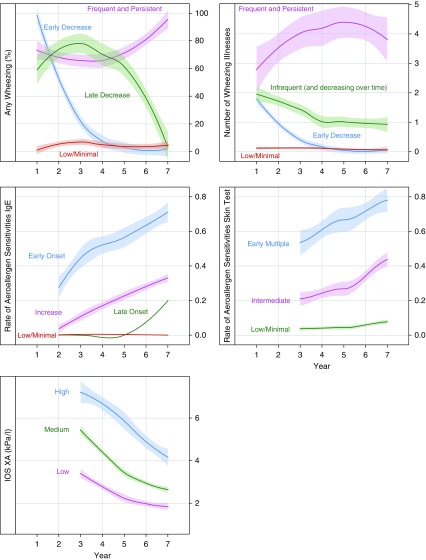
Methods: Data were collected prospectively from 442 children in the URECA (Urban Environment and Childhood Asthma) birth cohort through age 7 years, reflecting symptoms (wheezing), aeroallergen sensitization, pulmonary function, and body mass index. Latent class mixed models identified trajectories of wheezing, allergic sensitization, and pulmonary function. Cluster analysis defined nonoverlapping groups (termed phenotypes). Potential associations between phenotypes and early-life environmental exposures were examined.
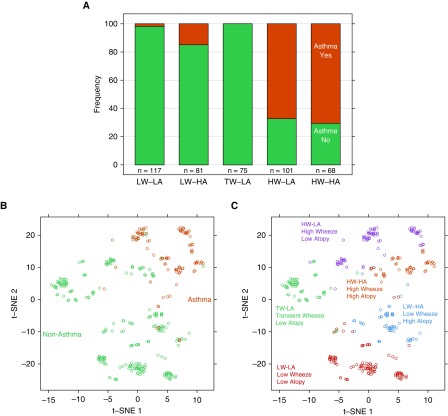
Measurements and main results: Five phenotypes were identified and mainly differentiated by patterns of wheezing and allergic sensitization (low wheeze/low atopy; low wheeze/high atopy; transient wheeze/low atopy; high wheeze/low atopy; high wheeze/high atopy). Asthma was most often present in the high-wheeze phenotypes, with greatest respiratory morbidity among children with frequent wheezing and allergic sensitization. These phenotypes differentially related to early-life exposures, including maternal stress and depression, antenatal environmental tobacco smoke, house dust microbiome, and allergen content (all P < 0.05). Prenatal smoke exposure, maternal stress, and depression were highest in the high-wheeze/low-atopy phenotype. The high-wheeze/high-atopy phenotype was associated with low household microbial richness and diversity. Early-life aeroallergen exposure was low in high-wheeze phenotypes.
Conclusions: Patterns of wheezing, allergic sensitization, and lung function identified five respiratory phenotypes among inner-city children. Early-life environmental exposure to stress, depression, tobacco smoke, and indoor allergens and microbes differentially associate with specific phenotypes.
Keywords: childhood asthma; environmental exposures; phenotypes.
Figures


Comment in
-
Respiratory Phenotypes during Childhood and Early-Life Exposures.Am J Respir Crit Care Med. 2019 Jan 1;199(1):7-9. doi: 10.1164/rccm.201807-1359ED. Am J Respir Crit Care Med. 2019. PMID: 30095995 No abstract available.
References
-
- Van Cleave J, Gortmaker SL, Perrin JM. Dynamics of obesity and chronic health conditions among children and youth. JAMA. 2010;303:623–630. - PubMed
-
- Crain EF, Weiss KB, Bijur PE, Hersh M, Westbrook L, Stein RE. An estimate of the prevalence of asthma and wheezing among inner-city children. Pediatrics. 1994;94:356–362. - PubMed
-
- Weiss KB, Gergen PJ, Crain EF. Inner-city asthma. The epidemiology of an emerging US public health concern. Chest. 1992;101(Suppl. 6):362S–367S. - PubMed
-
- Litonjua AA, Carey VJ, Weiss ST, Gold DR. Race, socioeconomic factors, and area of residence are associated with asthma prevalence. Pediatr Pulmonol. 1999;28:394–401. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 AI025496/AI/NIAID NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- UM1 AI114271/AI/NIAID NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- HHSN272200900052C/AI/NIAID NIH HHS/United States
- N01 AI025482/AI/NIAID NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- UM2 AI117870/AI/NIAID NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- P2C HD042849/HD/NICHD NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- HHSN272201000052I/AI/NIAID NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
