

Effect of partograph use on outcomes for women in spontaneous labour at term and their babies
- PMID: 30080256
- PMCID: PMC6513424
- DOI: 10.1002/14651858.CD005461.pub5
Effect of partograph use on outcomes for women in spontaneous labour at term and their babies
Abstract
Background: The partograph (sometimes known as partogram) is usually a pre-printed paper form on which labour observations are recorded. The aim of the partograph is to provide a pictorial overview of labour, and to alert midwives and obstetricians to deviations in maternal or fetal well-being and labour progress. Charts have traditionally contained pre-printed alert and action lines. An alert line, which is based on the slowest 10% of primigravid women's labours, signifies slow progress. An action line is placed a number of hours after the alert line (usually two or four hours) to prompt effective management of slow progress of labour.This review is an update of a review last published in 2013.
Objectives: The primary objective was to determine the effectiveness and safety of partograph use on perinatal and maternal morbidity and mortality. The secondary objective was to determine which partograph design is most effective for perinatal and maternal morbidity and mortality outcomes.
Search methods: We searched Cochrane Pregnancy and Childbirth's Trials Register (31 August 2017), ClinicalTrials.gov, the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (31 August 2017) and reference lists of retrieved studies.
Selection criteria: Randomised, cluster-randomised, and quasi-randomised controlled trials involving a comparison of partograph use with no partograph, or comparison between different partograph designs.
Data collection and analysis: Three review authors independently assessed eligibility, quality and extracted data. When one review author was also the trial author, the two remaining review authors assessed the studies independently. We assessed the evidence using the GRADE approach.
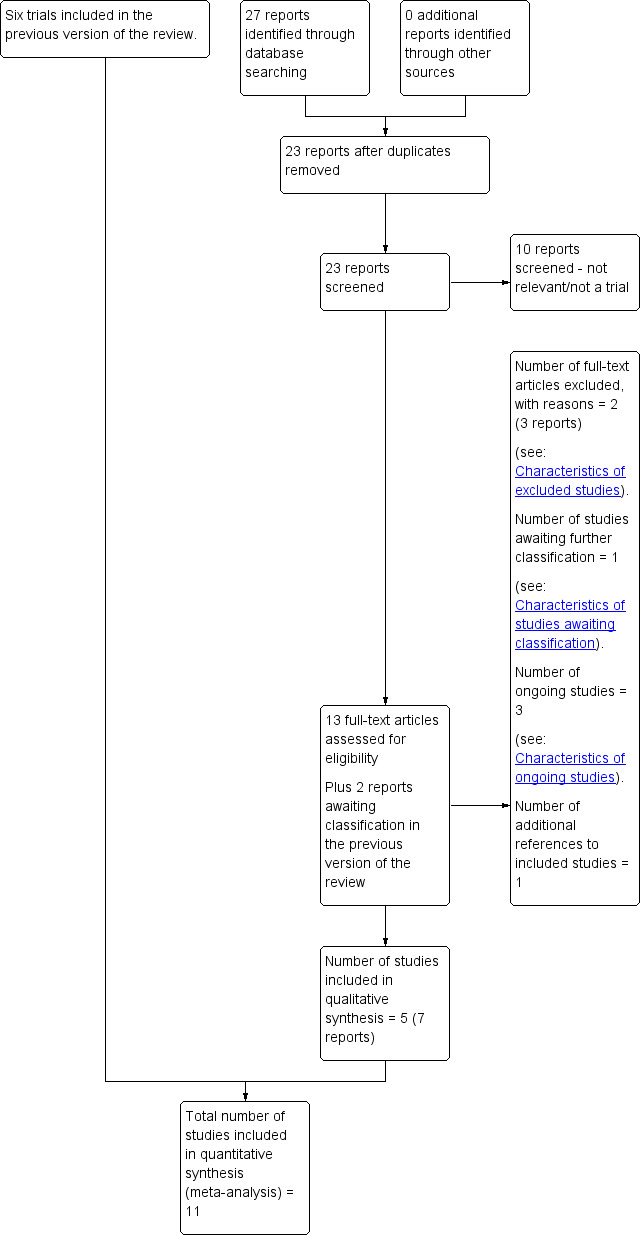
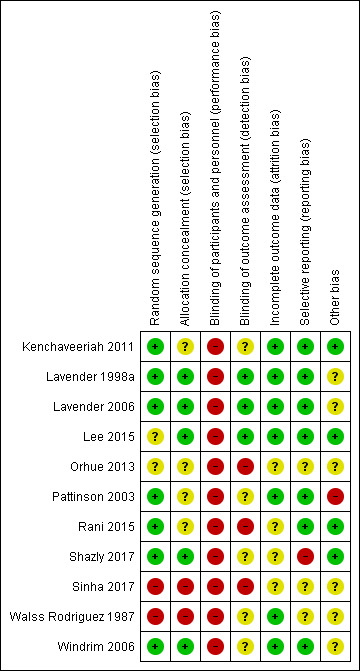
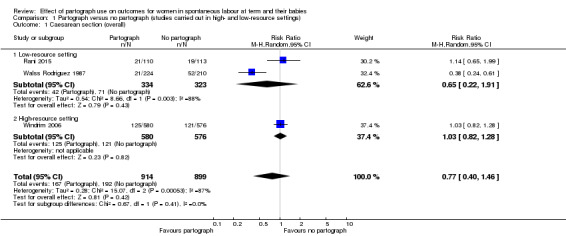
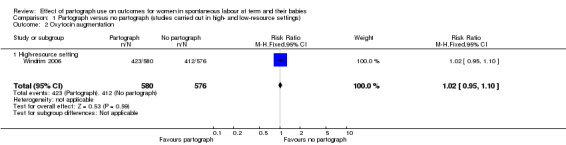
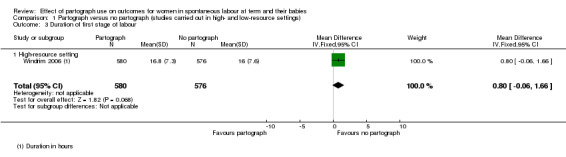
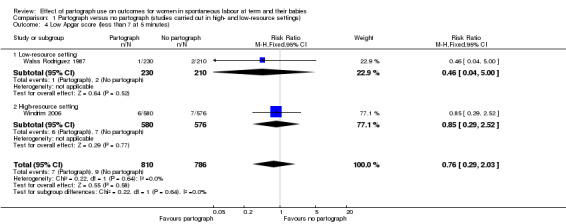
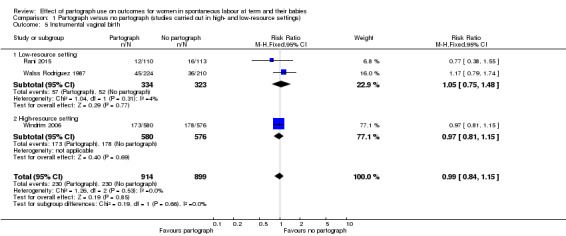
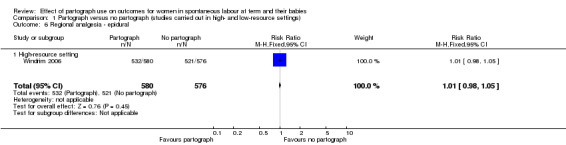
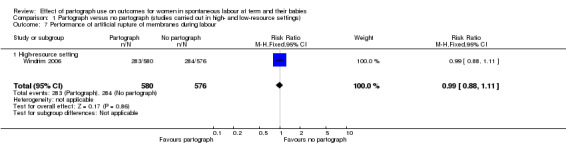
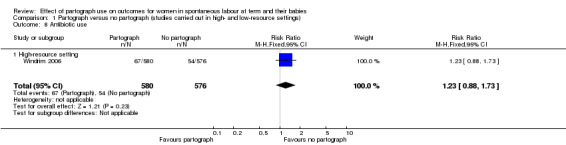
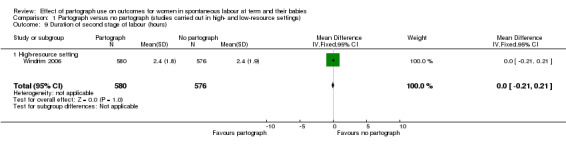
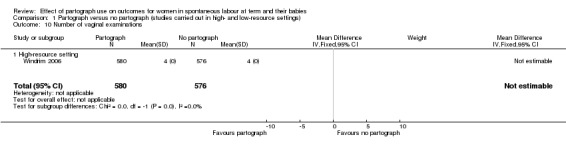
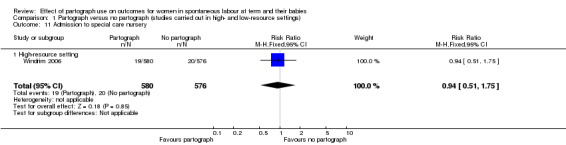
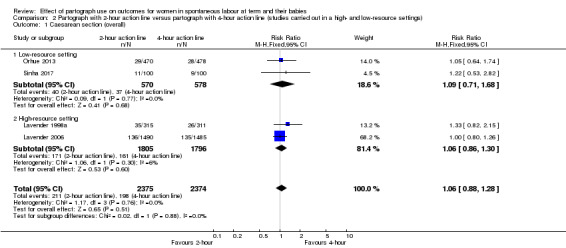
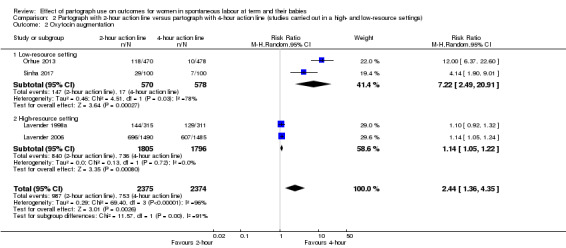
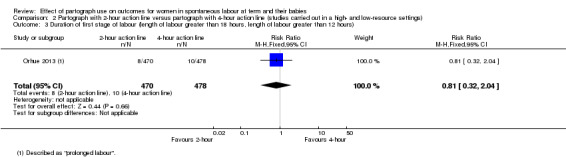
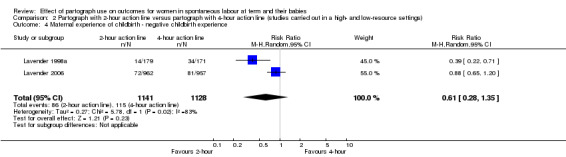
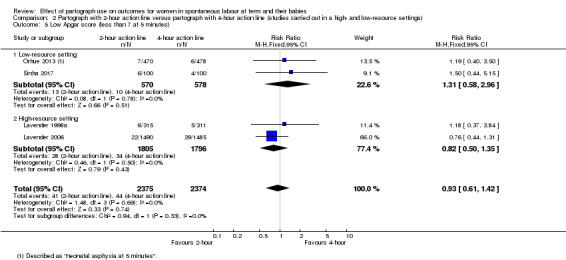
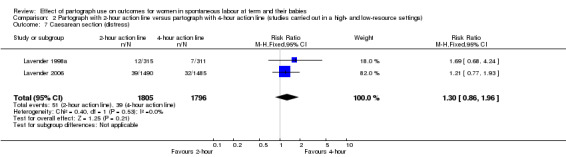
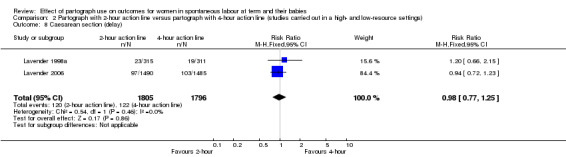
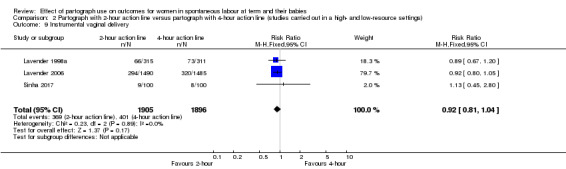
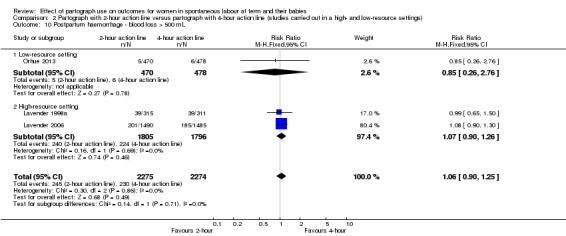
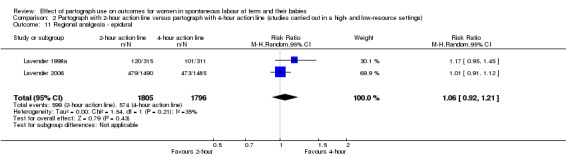
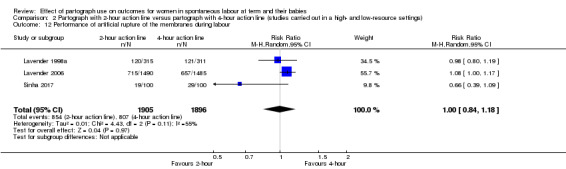
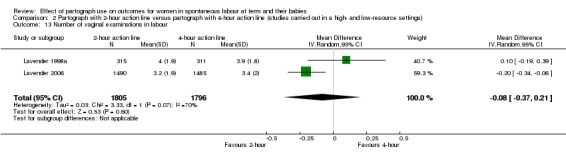
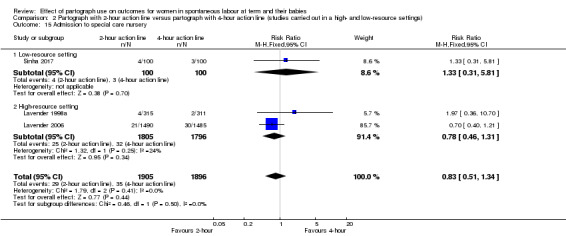
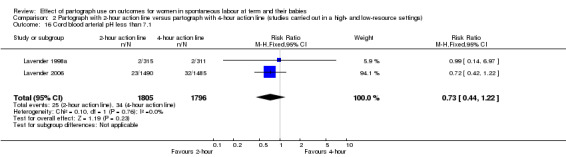
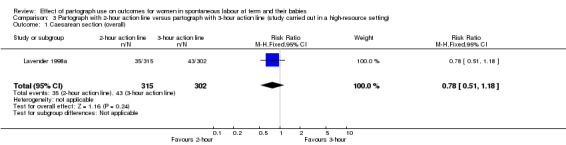
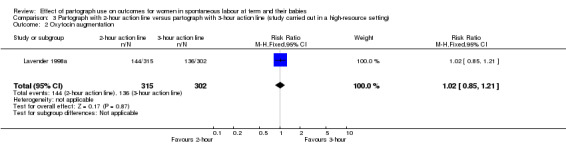
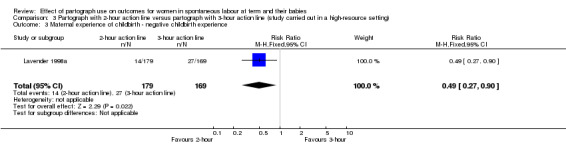
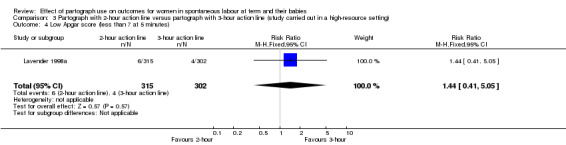
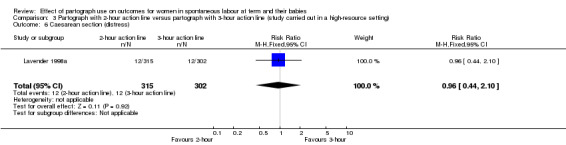
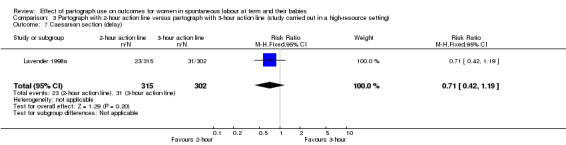
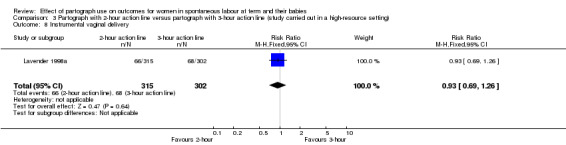
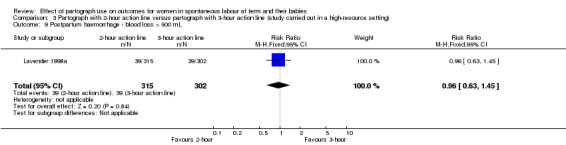
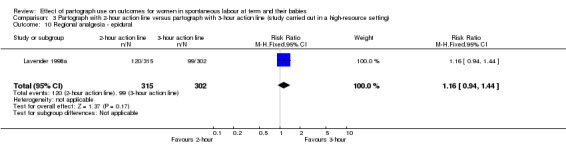
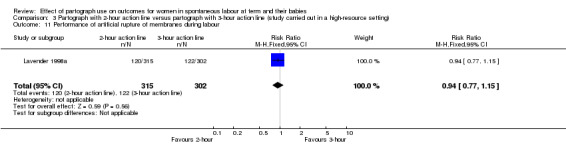
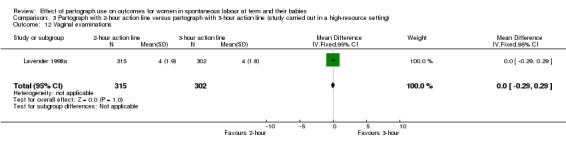
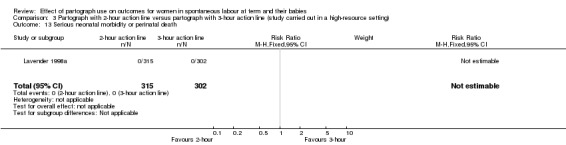
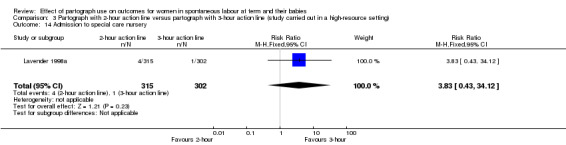
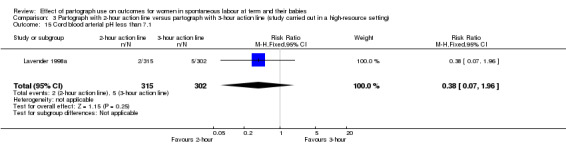
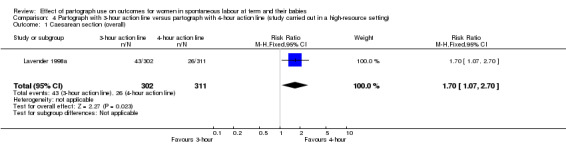
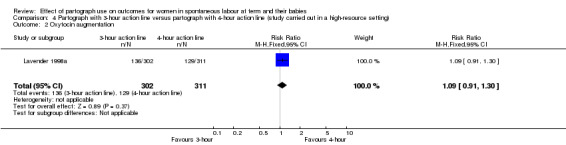
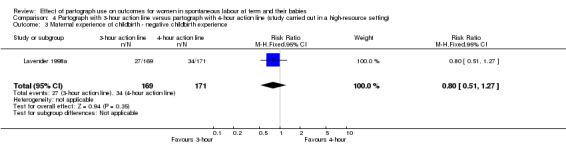
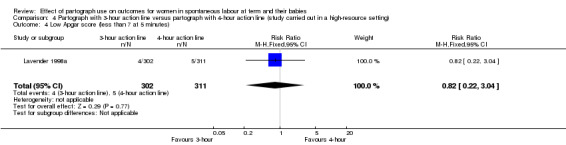
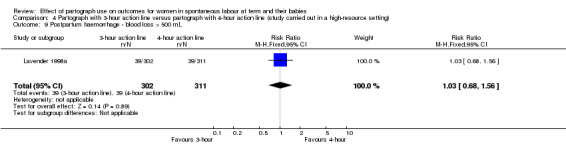
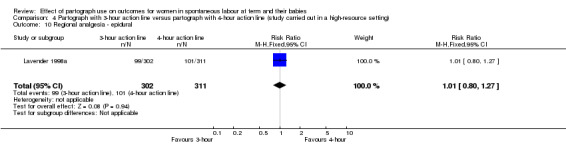
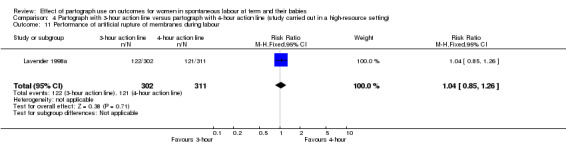
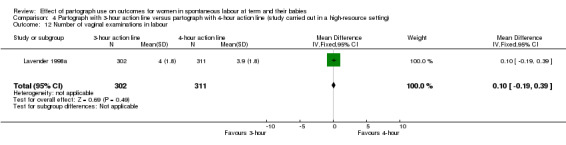
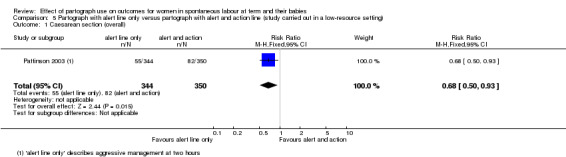
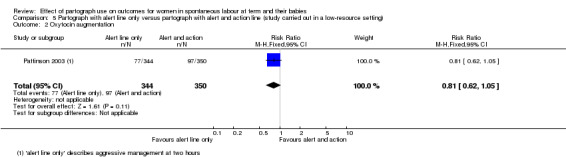
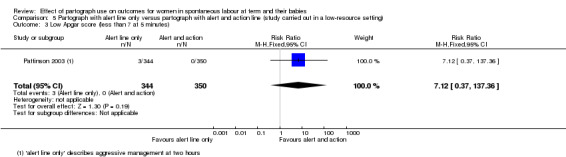
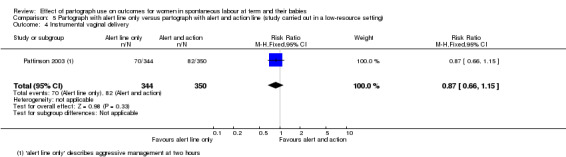
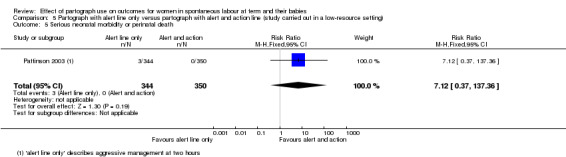
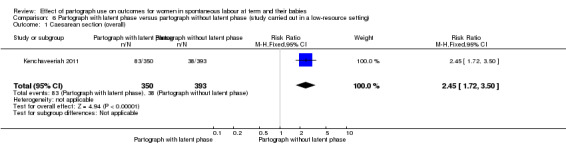
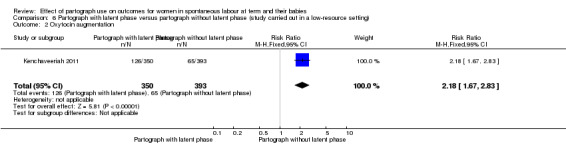
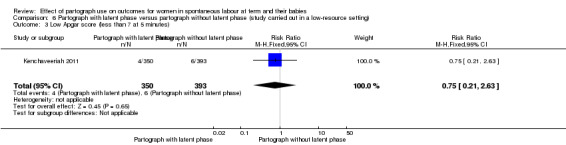
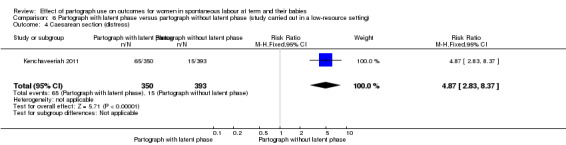
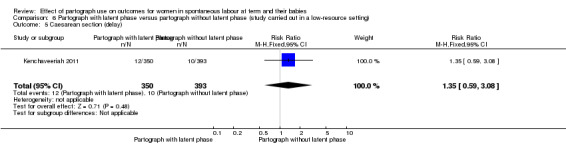
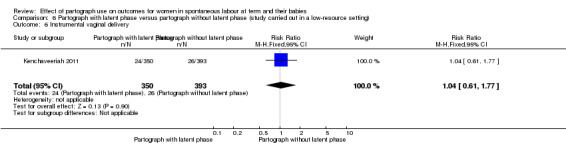
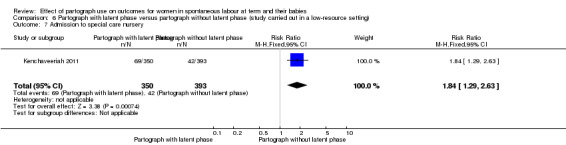
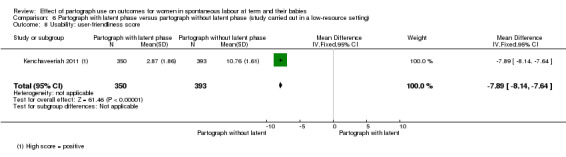
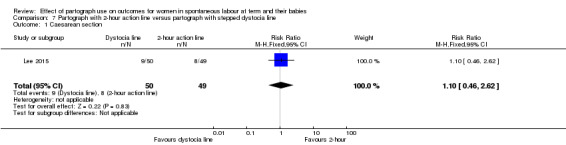
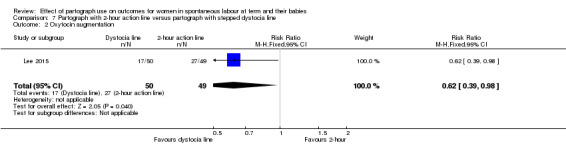
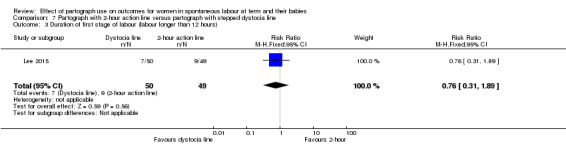
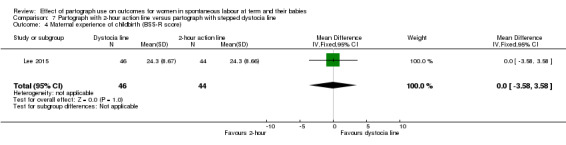
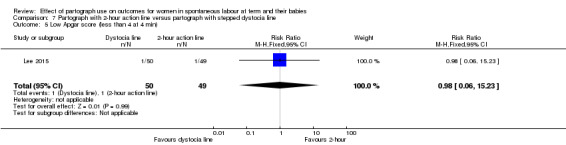
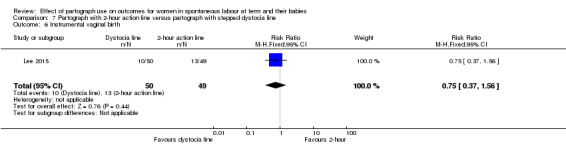
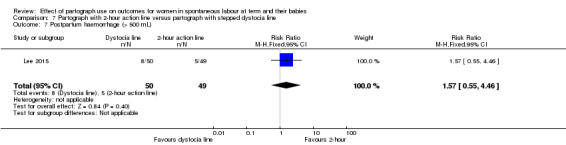
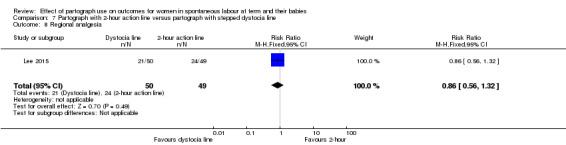
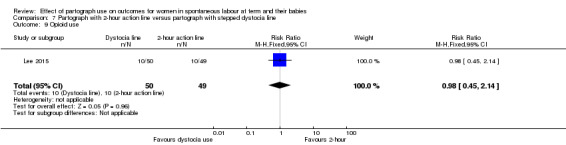
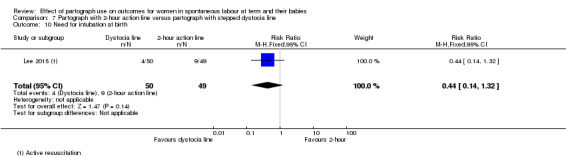
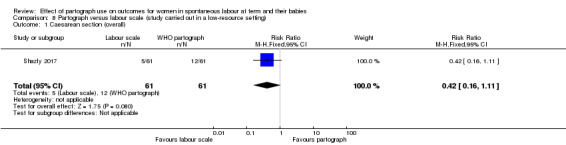
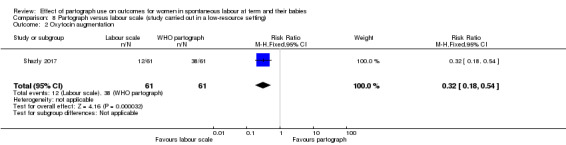
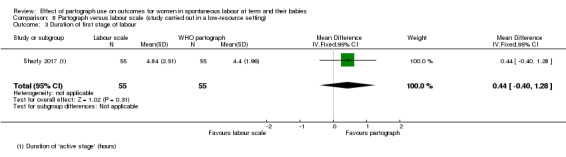
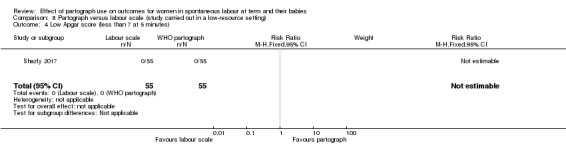
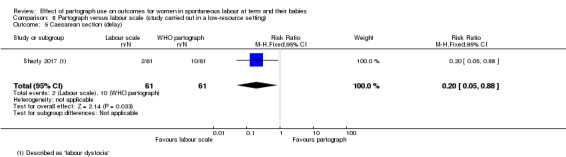
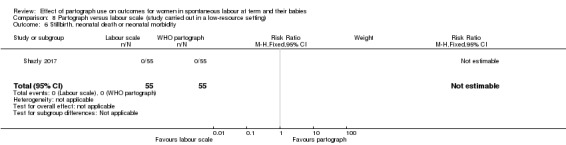
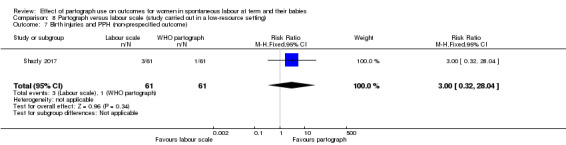
Main results: We have included 11 studies, involving 9475 women in this review; three studies assessed partograph use versus no partograph, seven assessed different partograph designs, and one assessed partograph use versus labour scale. Risk of bias varied in all studies. It was infeasible to blind staff or women to the intervention. Two studies did not adequately conceal allocation. Loss to follow-up was low in all studies. We assessed the evidence for partograph use versus no partograph using the GRADE approach; downgrading decisions were due to study design, inconsistency, indirectness, and imprecision of effect estimates.Most trials reported caesarean section rates and Apgar scores less than 7 at five minutes; all other outcomes were not consistently reported (e.g. duration of first stage of labour and maternal experience of childbirth).Partograph versus no partograph (3 trials, 1813 women)It is uncertain whether there is any clear difference between partograph use and no partograph in caesarean section rates (average risk ratio (RR) 0.77, 95% confidence interval (CI) 0.40 to 1.46; n = 1813; 3 trials; I² = 87%; very low-quality evidence); oxytocin augmentation (RR 1.02, 95% CI 0.95 to 1.10; n = 1156; 1 trial; moderate-quality evidence); duration of first stage of labour (mean difference (MD) 0.80 hours, 95% CI -0.06 to 1.66; n = 1156; 1 trial; low-quality evidence); or Apgar score less than 7 at five minutes (RR 0.76, 95% CI 0.29 to 2.03; n = 1596; 2 trials; I² = 87%; very low-quality evidence).Partograph with different placement of action lines (4 trials, 5051 women)When compared to a four-hour action line, women in the two-hour action line group were more likely to receive oxytocin augmentation (average RR 2.44, 95% CI 1.36 to 4.35; n = 4749; 4 trials; I² = 96%). There was no clear difference in caesarean section rates (RR 1.06, 95% CI 0.88 to 1.28; n = 4749; 4 trials); duration of first stage of labour (RR 0.81 hours, 95% CI 0.32 to 2.04; n = 948; 1 trial); maternal experience of childbirth (average RR 0.61, 95% CI 0.28 to 1.35; n = 2269; 2 trials; I² = 83%); or Apgar score less than 7 at five minutes (RR 0.93, 95% CI 0.61 to 1.42; n = 4749; 4 trials) between the two- and four-hour action line.The following comparisons only include data from single studies. Fewer women reported negative childbirth experiences in the two-hour action line group compared to the three-hour action line group (RR 0.49, 95% CI 0.27 to 0.90; n = 348; 1 trial). When we compared the three- and four-hour action line groups, the caesarean section rate was higher in the three-hour action line group (RR 1.70, 95% CI 1.07 to 2.70; n = 613; 1 trial). We did not observe any clear differences in any of the other outcomes in these comparisons.Partograph with alert line only versus partograph with alert and action line (1 trial, 694 women)The caesarean section rate was lower in the alert line only group (RR 0.68, 95% CI 0.50 to 0.93). There were no clear differences between groups for oxytocin augmentation, low Apgar score, instrumental vaginal birth and perinatal death.Partograph with latent phase (composite) versus partograph without latent phase (modified) (1 trial, 743 women)The caesarean section and oxytocin augmentation rates were higher in the partograph with a latent phase (RR 2.45, 95% CI 1.72 to 3.50; and RR 2.18, 95% CI 1.67 to 2.83, respectively). There were no clear differences between groups for oxytocin augmentation, and Apgar score less than 7 at five minutes.Partograph with two-hour action line versus partograph with stepped dystocia line (1 trial, 99 women)Fewer women received oxytocin augmentation in the dystocia line group (RR 0.62, 95% CI 0.39 to 0.98). We did not observe any clear differences in any of the other primary outcomes in this comparison.Partograph versus labour scale (1 trial, 122 women)The use of the partograph compared with the labour scale resulted in fewer women receiving oxytocin augmentation (RR 0.32, 95% CI 0.18 to 0.54), but did not produce any clear differences for any of the other primary outcomes.
Authors' conclusions: On the basis of the findings of this review, we cannot be certain of the effects of routine use of the partograph as part of standard labour management and care, or which design, if any, are most effective. Further trial evidence is required to establish the efficacy of partograph use per se and its optimum design.
Conflict of interest statement
Tina Lavender: was investigator of two trials included in this review (Lavender 1998a; Lavender 2006); therefore, she was not involved with evaluating these studies. No other relevant conflicts of interest.
Anna Cuthbert: is employed by the University of Liverpool as a Research Associate with Cochrane Pregnancy and Childbirth. Her employment is supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. She had no involvement with the editorial processes for this review update.
Rebecca Smyth: none known.
Figures

Update of
-
Effect of partogram use on outcomes for women in spontaneous labour at term.Cochrane Database Syst Rev. 2013 Jul 10;(7):CD005461. doi: 10.1002/14651858.CD005461.pub4. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2018 Aug 06;8:CD005461. doi: 10.1002/14651858.CD005461.pub5. PMID: 23843091 Updated.
References
References to studies included in this review
Kenchaveeriah 2011 {published data only}
Lavender 1998a {published and unpublished data}
-
- Lavender T, Walkinshaw S, Alfirevic Z. Partogram action line study: a randomised trial. British Journal of Obstetrics and Gynaecology 1998;105:976‐80. - PubMed
-
- Lavender T, Walkinshaw SA, Walton I. A prospective study of women's views of factors contributing to a positive birth experience. Midwifery 1999;15:40‐6. - PubMed
-
- Lavender T, Wallymahmed AH, Walkinshaw SA. Managing labor using partograms with different action lines: a prospective study of womens views. Birth 1999;26:89‐96. - PubMed
Lavender 2006 {published and unpublished data}
-
- ISRCTN78346801. Partogram Action Line Study (PALS2). isrctn.com/ISRCTN78346801 (first received 6 July 2005).
-
- Lavender T, Alfirevic Z, Walkinshaw S. Effect of different partogram action lines on birth outcomes. Obstetrics & Gynecology 2006;108:295‐302. - PubMed
Lee 2015 {published data only}
-
- ACTRN12614000786695. A pilot randomised controlled trial to determine the effect of a physiological (step) versus a standard action (slope) labour progress lines on the rate of spontaneous vaginal birth amongst low risk women in labour for the first time [For women in labour for the first time does a partograph with a graduated dystocia line compared to a standard sloping action line increase the likelihood of a spontaneous vaginal birth]. anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12614000786695 (first received 7 July 2014).
-
- ACTRN12615000445572. A pilot randomised controlled trial to determine the effect of two designs of partographs, including labour progress lines, on the rate of spontaneous vaginal birth amongst low risk women in labour for the first time: The Partograph Trial [For women in labour for the first time does a partograph with a graduated dystocia line compared to a standard sloping action line increase the likelihood of a spontaneous vaginal birth: Pilot Partograph study 2]. anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12615000445572 (first received 13 April 2015).
Orhue 2013 {published data only}
-
- Orhue A, Iribhogbe I. Outcome of a protocol for the use of the partograph as a decision‐making algorithm for the prevention of prolonged labor. 1st FIGO African Regional Conference of Gynecology and Obstetrics; 2013 Oct 2‐5; Addis Ababa, Ethiopia. 2013.
Pattinson 2003 {published data only}
-
- Pattinson RC, Howarth GR, Mdluli W, Macdonald AP, Makin JD, Funk M. Aggressive or expectant management of labour: a randomised trial. BJOG: an international journal of obstetrics and gynaecology 2003;110:457‐61. - PubMed
Rani 2015 {published data only}
-
- Rani J, Sharma D, Sehgal A. Role of partogram in high risk pregnancies: an experience at a tertiary centre. Archives of Gynecology & Obstetrics 2015;291(1):73‐8. - PubMed
Shazly 2017 {published data only}
-
- NCT02486822. The management of spontaneous labour in primigravida (SLIP): labor scale versus WHO partograph [Labor scale versus WHO partograph in the management of labor]. clinicaltrials.gov/ct2/show/record/NCT02486822 (first received 24 June 2015).
-
- Shazly SA, Tolba S, Abbas AM, Nassr AA. Management of spontaneous labor in primigravidae: labor scale versus who partograph (SLiP trial). American Journal of Obstetrics and Gynecology 2017;216(1):S510‐1, Abstract no: 894. - PubMed
Sinha 2017 {published data only}
-
- Sinha D, Shrivastava S, Shrivastava S. A comparative study of 4‐hour versus 2‐hour action line on WHO modified partograph. International Journal of Research in Medical Sciences 2017;5(3):876‐9.
Walss Rodriguez 1987 {published data only}
-
- Walss‐Rodriguez RJ, Gudino‐Ruiz F, Tapia‐Rodriguez S. Comparative study between Friedman's partogram and conventional descriptive partogram. Ginecologia y Obstetricia de Mexico 1987;55:318‐22. - PubMed
Windrim 2006 {published and unpublished data}
-
- Windrim R, Seaward G, Hodnett E, Akoury H, Kingdom J, Salenieks ME, et al. A randomized controlled trial of a bedside partogram in the active management of primiparous labour. Journal of Obstetrics and Gynaecology Canada: JOGC 2006;29(1):27‐34. - PubMed
References to studies excluded from this review
Ajoodani 2011 {published data only}
-
- Ajoodani Z, Heidari P, Nasrollahi S. Assessment of the results of using partogram in labor management. Iranian Journal of Obstetrics, Gynecology and Infertility 2011;14(2):20‐7.
-
- IRCT2012122811911N1. Labor management based on partogram. en.search.irct.ir/view/11959 (first received 24 September 2003).
Cartmill 1992 {published data only}
-
- Cartmill R, Thornton J. Effect of presentation of partogram information on obstetric decision‐making. Lancet 1992;339:1520‐2. - PubMed
Fahdhy 2005 {published data only}
-
- Fahdhy M, Chongsuvivatwong V. Evaluation of World Health Organization partograph implementation by midwives for maternity home birth in Medan, Indonesia. Midwifery 2005;21:301‐10. - PubMed
Hamilton 2001 {published data only}
-
- Hamilton E, Platt RW, Gauthier RJ, McNamara H, Miner L, Rothenberg S, et al. A multicenter trial of individualized labor curves and cesarean rates. American Journal of Obstetrics and Gynecology Vol. 185, issue 6 Suppl:S103.
Hamilton 2004 {published data only}
-
- Hamilton E, Platt R, Gauthier R, McNamara H, Miner L, Rothenberg S, et al. The effect of computer‐assisted evaluation of labor on cesarean rates. Journal for Healthcare Quality 2004;26(1):37‐44. - PubMed
Kogovsek 2000 {published data only}
-
- Kogovsek U, Assejev V, Novak‐Antolic Z. Partogram presentation and the outcome of labour and delivery. Effectiveness of prenatal care in Slovenia; 2000 June 1‐3; Slovenia. 2000:125‐32.
Mathews 2007 {published data only}
-
- Mathews JE, Rajaratnam A, George A, Mathai M. Comparison of two World Health Organization partographs. International Journal of Gynecology & Obstetrics 2007;96(2):147‐50. - PubMed
WHO 1994 {published data only}
-
- Anonymous. World Health Organization partograph in management of labour. World Health Organization Maternal Health and Safe Motherhood Programme. Lancet 1994;343(8910):1399‐404. - PubMed
References to studies awaiting assessment
NCT02911272 {published data only}
-
- NCT02911272. Best partograph action line to prevent prolonged labour (partograph). clinicaltrials.gov/show/NCT02911272 (first received 14 September 2016).
References to ongoing studies
NCT02714270 {published data only}
-
- NCT02714270. A randomized clinical trial of paperless versus modified World Health Organization partograph in management of first stage of labour [Paperless partograph for management of low risk labour]. clinicaltrials.gov/ct2/show/NCT02714270 (first received 16 March 2016).
NCT02741141 {published data only}
-
- NCT02741141. A comparative study of the effect of two partographs on the cesarean section rate in women in spontaneous labour (PARTODYS). clinicaltrials.gov/show/NCT02741141 (first received 12 January 2016).
NTR5543 {published data only}
-
- NTR5543. Randomized controlled trial comparing the currently used Friedman partogram with a four hour action line to the newly developed simple partogram, based on the 95th percentile normogram of the consortium on safe labor to evaluate early versus delayed cesarean section. trialregister.nl/trialreg/admin/rctview.asp?TC=5543 (first received 4 October 2015).
Additional references
Agarwal 2013
Bedwell 2017
Bosse 2002
-
- Bosse G, Massawe S, Jahn A. The partograph in daily practice: It's quality that matters. International Journal of Gynecology and Obstetrics 2002;77(3):243‐4. - PubMed
Downe 2013
Fatusi 2007
-
- Fatusi AO, Makinde ON, Adetemi AB. Evaluation of health workers' training in use of the partogram. International Journal of Gynecology and Obstetrics 2007;100(1):41‐4. - PubMed
Fawole 2008
-
- Fawole AO, Hunyinbo KI, Adekanle DA. Knowledge and utilization of the partograph among obstetric care givers in South West Nigeria. African Journal of Reproductive Health 2008;12(1):22‐9. - PubMed
Fistula Care 2012
-
- Fistula Care and Maternal Health Task Force. Revitalizing the partograph: does the evidence support a global call to action?. Report of an Expert Meeting; 2011 November 15‐16; New York (NY) (accessed 12 June 2012). New York (NY) www.fistulacare.org/pages/pdf/program‐reports/EngenderHealth‐Fistula‐Car... EngenderHealth/Fistula Care, 2012.
Friedman 1954
-
- Friedman E. Graphic analysis of labour. American Journal of Obstetrics and Gynecology 1954;68:1568‐75. - PubMed
Groeschel 2001
-
- Groeschel N, Glover P. The partograph. Used daily but rarely questioned. Australian Journal of Midwifery 2001;14:22‐7. - PubMed
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Lavender 1998b
-
- Lavender T, Alfirevic Z, Walkinshaw S. Partogram action line study: a randomised trial. British Journal of Obstetrics and Gynaecology 1998;105(9):976‐80. - PubMed
Lavender 1999
-
- Lavender T, Malcolmson L. Is the partogram a help or a hindrance?. Practising Midwife 1999;2:23‐7. - PubMed
Lavender 2011
-
- Lavender T, Omoni G, Lee K, Wakasiaka S, Watiti J, Mathai M. Student nurses experiences of using the partograph in labour wards in Kenya: A qualitative study. African Journal of Midwifery and Women’s Health 2011;5(3):117‐22.
Lennox 1995
-
- Lennox CE, Kwast BE. The partograph in community obstetrics. Tropical Doctor 1995;25:56‐63. - PubMed
Neilson 2003
-
- Neilson J, Lavender T, Quenby S, Wray S. Obstructed labour. British Medical Bulletin 2003;67:191‐204. - PubMed
Nystedt 2014
Oladapo 2017
-
- Oladapo OT, Diaz V, Bonet M, Abalos E, Thwin SS, Souza H, et al. Cervical dilatation patterns of 'low‐risk' women with spontaneous labour and normal perinatal outcomes: a systematic review. BJOG: an international journal of obstetrics and gynaecology 2017 Sep 11 [Epub ahead of print]. [DOI: 10.1111/1471-0528.14930.] - DOI - PMC - PubMed
Ollerhead 2014
Orhue 2012
-
- Orhue AAE, Aziken ME, Osemwenkha AP. Partograph as a tool for team work management of spontaneous labor. Nigerian Journal of Clinical Practice 2012;15:1‐8. - PubMed
Pawson 2004
-
- Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist synthesis: an introduction. ESRC Research Methods Programme ‐ University of Manchester 2004.
Philpott 1972a
Philpott 1972b
-
- Philpott RH, Castle WM. Cervicographs in the management of labour in primigravidae. Journal of Obstetrics and Gynaecology of the British Commonwealth 1972;79:592‐8. - PubMed
Philpott 1972c
-
- Philpott RH, Castle WM. Cervicographs in the management of labour in primigravidae. Journal of Obstetrics and Gynaecology of the British Commonwealth 1972;79:599‐602. - PubMed
Rakotonirina 2013
-
- Rakotonirina JE, Randrianantenainjatovo CH, Elyan Edwige BB, Dorasse R, Rakotomanga J, Rakotovao JH. Assessment of the use of partographs in the region of Analamanga. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 2013;2:257‐62.
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rotich 2011
-
- Rotich E, Maina L, Njihia A, Christensson K. Evaluating partograph use at two main referral hospitals in Kenya. African Journal of Midwifery and Women's Health 2011;5:21‐4.
Shazly 2014
-
- Shazly SAM, Embaby LHO, Ali SS. The labour scale – assessment of the validity of a novel labour chart: A pilot study. Australian and New Zealand Journal of Obstetrics and Gynaecology 2014;54:322‐6. - PubMed
Tay 1996
-
- Tay SK, Yong TT. Visual effect of partogram designs on the management and outcome of labour. Australian and New Zealand Journal of Obstetrics and Gynaecology 1996;36:395‐400. - PubMed
Walraven 1994
-
- Walraven GE. WHO partograph. Lancet 1994;344:617. - PubMed
Walsh 1994
-
- Walsh D. Management of progress in the first stage of labour. Midwives Chronicle and Nursing Notes 1994;3:84‐8. - PubMed
WHO 2003
-
- World Health Organization. Pregnancy, Childbirth, Postpartum and Newborn care: A Guide for Essential Practice. Geneva: World Health Organization, 2003. - PubMed
References to other published versions of this review
Lavender 2005
-
- Lavender T, O'Brien P, Hart A. Effect of partogram use on outcomes for women in spontaneous labour at term. Cochrane Database of Systematic Reviews 2005, Issue 3. [DOI: 10.1002/14651858.CD005461] - DOI
Lavender 2008
Lavender 2012
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical