

Methotrexate mechanism in treatment of rheumatoid arthritis
- PMID: 30081197
- PMCID: PMC6360124
- DOI: 10.1016/j.jbspin.2018.07.004
Methotrexate mechanism in treatment of rheumatoid arthritis
Abstract
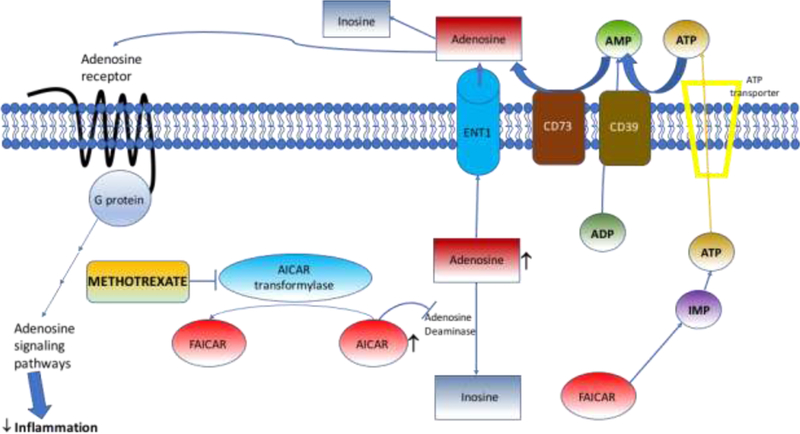
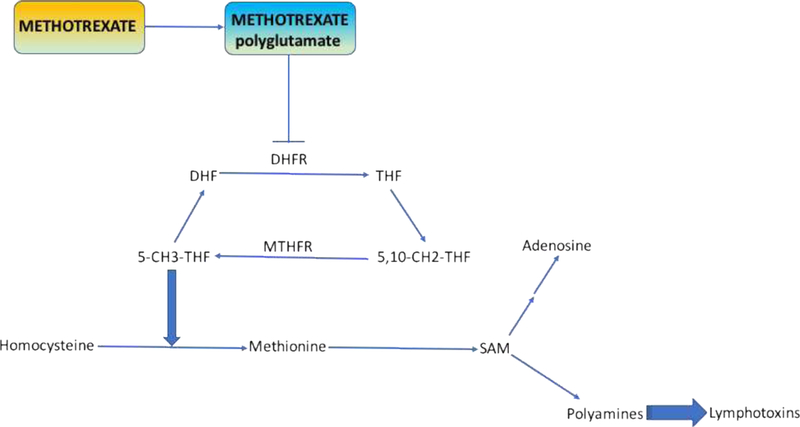
Methotrexate has been used in treatment of rheumatoid arthritis (RA) since the 1980s and to this day is often the first line medication for RA treatment. In this review, we examine multiple hypotheses to explain the mechanism of methotrexate efficacy in RA. These include folate antagonism, adenosine signaling, generation of reactive oxygen species (ROS), decrease in adhesion molecules, alteration of cytokine profiles, and polyamine inhibition amongst some others. Currently, adenosine signaling is probably the most widely accepted explanation for the methotrexate mechanism in RA given that methotrexate increases adenosine levels and on engagement of adenosine with its extracellular receptors an intracellular cascade is activated promoting an overall anti-inflammatory state. In addition to these hypotheses, we examine the mechanism of methotrexate in RA from the perspective of its adverse effects and consider some of the newer genetic markers of methotrexate efficacy and toxicity in RA. Lastly, we briefly discuss the mechanism of additive methotrexate in the setting of TNF-α inhibitor treatment of RA. Ultimately, finding a clear explanation for the pathway and mechanism leading to methotrexate efficacy in RA, there may be a way to formulate more potent therapies with fewer side effects.
Keywords: Adenosine A2A receptor; Adenosine signaling; Methotrexate; Methotrexate efficacy; Methotrexate toxicity; Rheumatoid arthritis.
Copyright © 2018 Société française de rhumatologie. Published by Elsevier Masson SAS. All rights reserved.
Figures

References
-
- Weinblatt ME, Coblyn JS, Fox DA, Fraser PA, Holdsworth DE, Glass DN, et al. Efficacy of low-dose methotrexate in rheumatoid arthritis. N Engl J Med. 1985;312(13):818–22. - PubMed
-
- Whittle SL, Hughes RA. Folate supplementation and methotrexate treatment in rheumatoid arthritis: a review. Rheumatology (Oxford). 2004;43(3):267–71. - PubMed
-
- Pichlmeier U, Heuer KU. Subcutaneous administration of methotrexate with a prefilled autoinjector pen results in a higher relative bioavailability compared with oral administration of methotrexate. Clin Exp Rheumatol. 2014;32(4):563–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
