

Clinically prevalent mutations in Mycobacterium tuberculosis alter propionate metabolism and mediate multidrug tolerance
- PMID: 30082724
- PMCID: PMC6233875
- DOI: 10.1038/s41564-018-0218-3
Clinically prevalent mutations in Mycobacterium tuberculosis alter propionate metabolism and mediate multidrug tolerance
Abstract
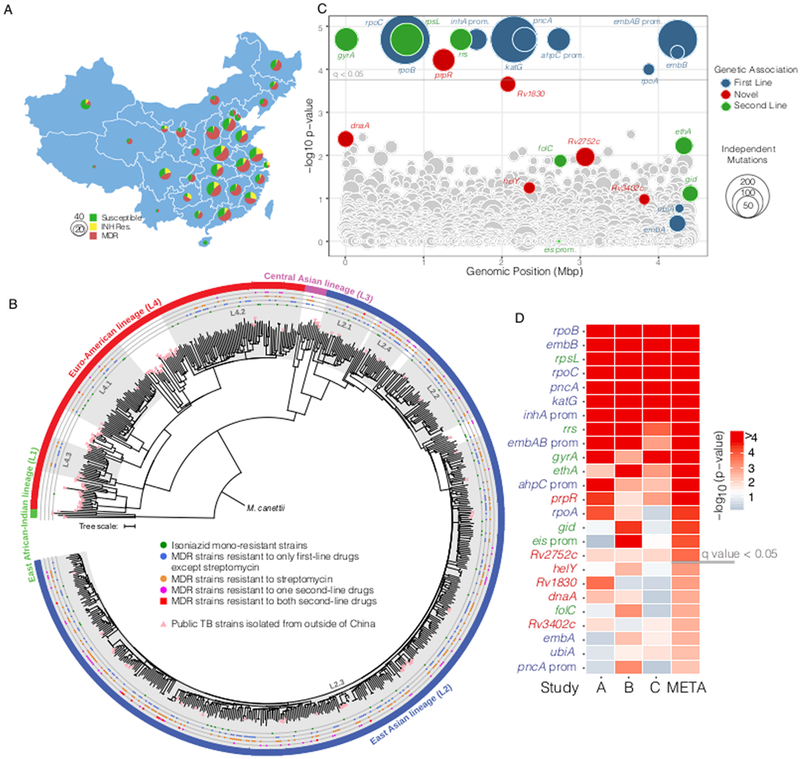
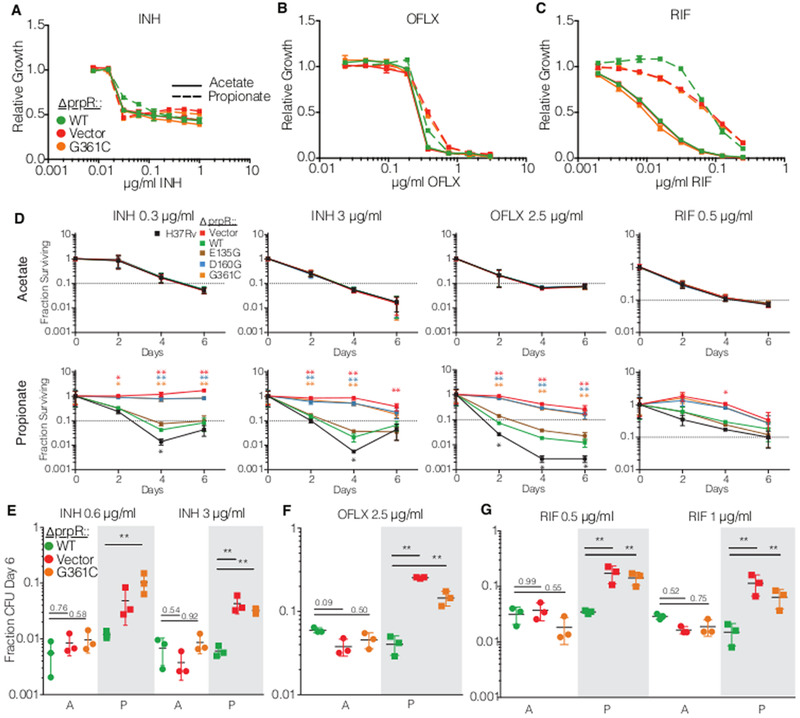
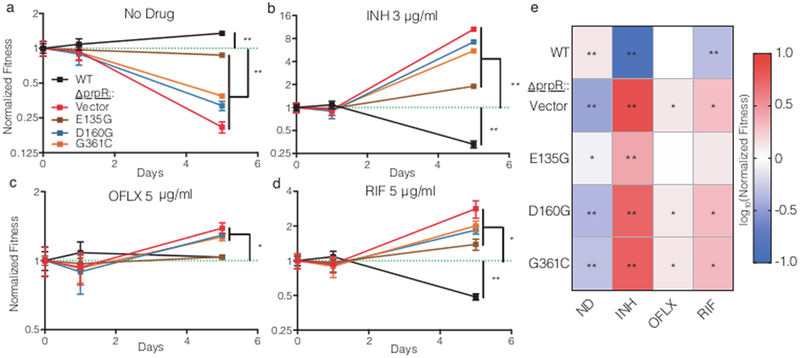
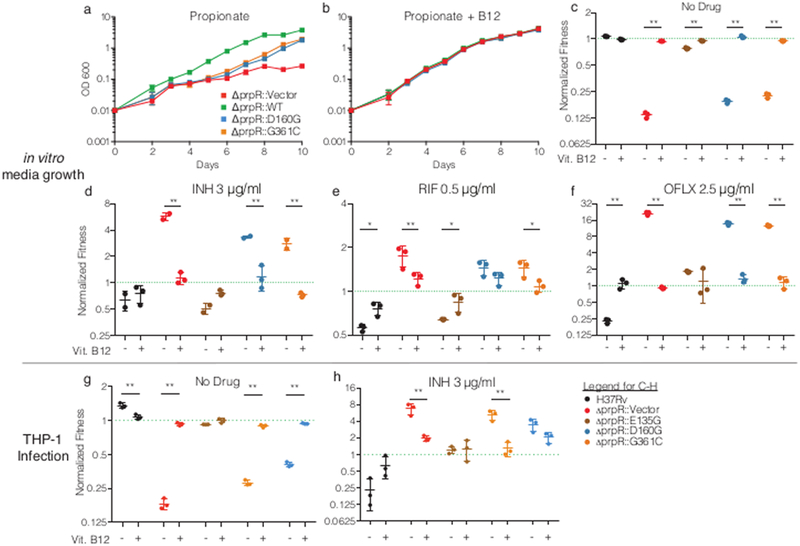
The global epidemic of drug-resistant tuberculosis is a catastrophic example of how antimicrobial resistance is undermining the public health gains made possible by combination drug therapy. Recent evidence points to unappreciated bacterial factors that accelerate the emergence of drug resistance. In a genome-wide association study of Mycobacterium tuberculosis isolates from China, we find mutations in the gene encoding the transcription factor prpR enriched in drug-resistant strains. prpR mutations confer conditional drug tolerance to three of the most effective classes of antibiotics by altering propionyl-CoA metabolism. prpR-mediated drug tolerance is carbon-source dependent, and while readily detectable during infection of human macrophages, is not captured by standard susceptibility testing. These data define a previously unrecognized and clinically prevalent class of M. tuberculosis variants that undermine antibiotic efficacy and drive drug resistance.
Figures

Comment in
-
TB drug susceptibility is more than MIC.Nat Microbiol. 2018 Sep;3(9):971-972. doi: 10.1038/s41564-018-0226-3. Nat Microbiol. 2018. PMID: 30143801 No abstract available.
References
-
- WHO. Global Tuberculosis Report. 2017 http://www.who.int/tb/publications/global_report/gtbr2017_main_text.pdf.
-
- Gegia M, Winters N, Benedetti A, van Soolingen D & Menzies D Treatment of isoniazid-resistant tuberculosis with first-line drugs: a systematic review and meta-analysis. Lancet Infect Dis 17, 223–234 (2017). - PubMed
-
- Weis SE et al. The effect of directly observed therapy on the rates of drug resistance and relapse in tuberculosis. N. Engl. J. Med 330, 1179–84 (1994). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
