

Gastric neuroendocrine neoplasm with late liver metastasis
- PMID: 30083348
- PMCID: PMC6075368
- DOI: 10.1530/EDM-18-0048
Gastric neuroendocrine neoplasm with late liver metastasis
Abstract
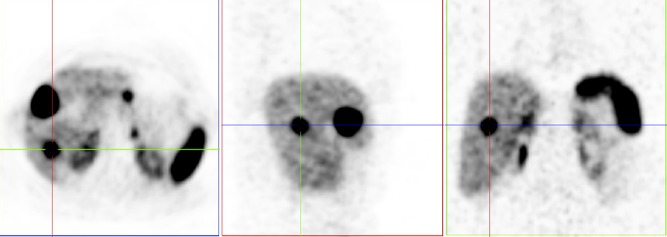
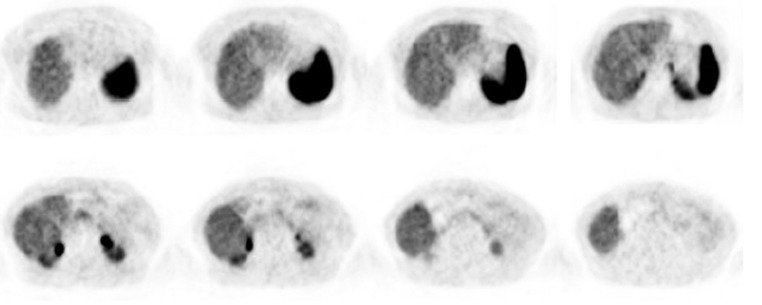
Gastric neuroendocrine neoplasms (GNENs) are classified into three types according to their aetiology. We present a clinical case of a female patient of 66 years and a well-differentiated (grade 2), type 3 GNEN with late liver metastasis (LM). The patient underwent surgical excision of a gastric lesion at 50 years of age, without any type of follow-up. Sixteen years later, she was found to have a neuroendocrine tumour (NET) metastatic to the liver. The histological review of the gastric lesion previously removed confirmed that it was a NET measuring 8 mm, pT1NxMx (Ki67 = 4%). 68Ga-DOTANOC PET/CT reported two LM and a possible pancreatic tumour/gastric adenopathy. Biopsies of the lesion were repeatedly inconclusive. She had a high chromogranin A, normal gastrin levels and negative anti-parietal cell and intrinsic factor antibodies, which is suggestive of type 3 GNEN. She underwent total gastrectomy and liver segmentectomies (segment IV and VII) with proven metastasis in two perigastric lymph nodes and both with hepatic lesions (Ki67 = 5%), yet no evidence of local recurrence. A 68Ga-DOTANOC PET/CT was performed 3 months after surgery, showing no tumour lesions and normalisation of CgA. Two years after surgery, the patient had no evidence of disease. This case illustrates a rare situation, being a type 3, well-differentiated (grade 2) GNEN, with late LM. Despite this, it was possible to perform surgery with curative intent, which is crucial in these cases, as systemic therapies have limited efficacy. We emphasise the need for extended follow-up in these patients.
Learning points: GNENs have a very heterogeneous biological behaviour.Clinical distinction between the three types of GNEN is essential to plan the correct management strategy.LMs are rare and more common in type 3 and grade 3 GNEN.Adequate follow-up is crucial for detection of disease recurrence.Curative intent surgery is the optimal therapy for patients with limited and resectable LM, especially in well-differentiated tumours (grade 1 and 2).
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
