

Diagnosis of Kawasaki Disease Using a Minimal Whole-Blood Gene Expression Signature
- PMID: 30083721
- PMCID: PMC6233768
- DOI: 10.1001/jamapediatrics.2018.2293
Diagnosis of Kawasaki Disease Using a Minimal Whole-Blood Gene Expression Signature
Abstract
Importance: To date, there is no diagnostic test for Kawasaki disease (KD). Diagnosis is based on clinical features shared with other febrile conditions, frequently resulting in delayed or missed treatment and an increased risk of coronary artery aneurysms.
Objective: To identify a whole-blood gene expression signature that distinguishes children with KD in the first week of illness from other febrile conditions.
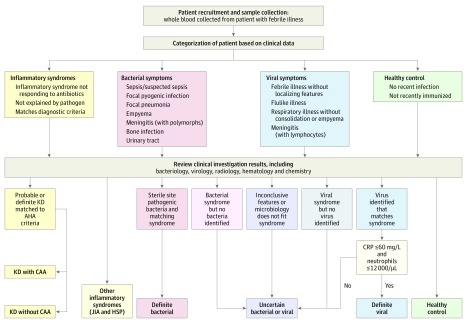
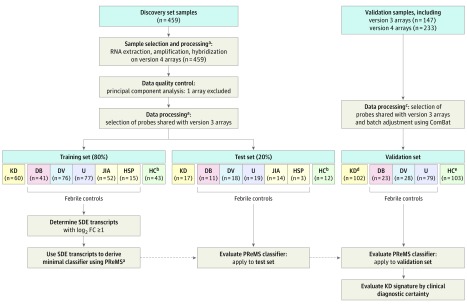
Design, setting, and participants: The case-control study comprised a discovery group that included a training and test set and a validation group of children with KD or comparator febrile illness. The setting was pediatric centers in the United Kingdom, Spain, the Netherlands, and the United States. The training and test discovery group comprised 404 children with infectious and inflammatory conditions (78 KD, 84 other inflammatory diseases, and 242 bacterial or viral infections) and 55 healthy controls. The independent validation group comprised 102 patients with KD, including 72 in the first 7 days of illness, and 130 febrile controls. The study dates were March 1, 2009, to November 14, 2013, and data analysis took place from January 1, 2015, to December 31, 2017.
Main outcomes and measures: Whole-blood gene expression was evaluated using microarrays, and minimal transcript sets distinguishing KD were identified using a novel variable selection method (parallel regularized regression model search). The ability of transcript signatures (implemented as disease risk scores) to discriminate KD cases from controls was assessed by area under the curve (AUC), sensitivity, and specificity at the optimal cut point according to the Youden index.
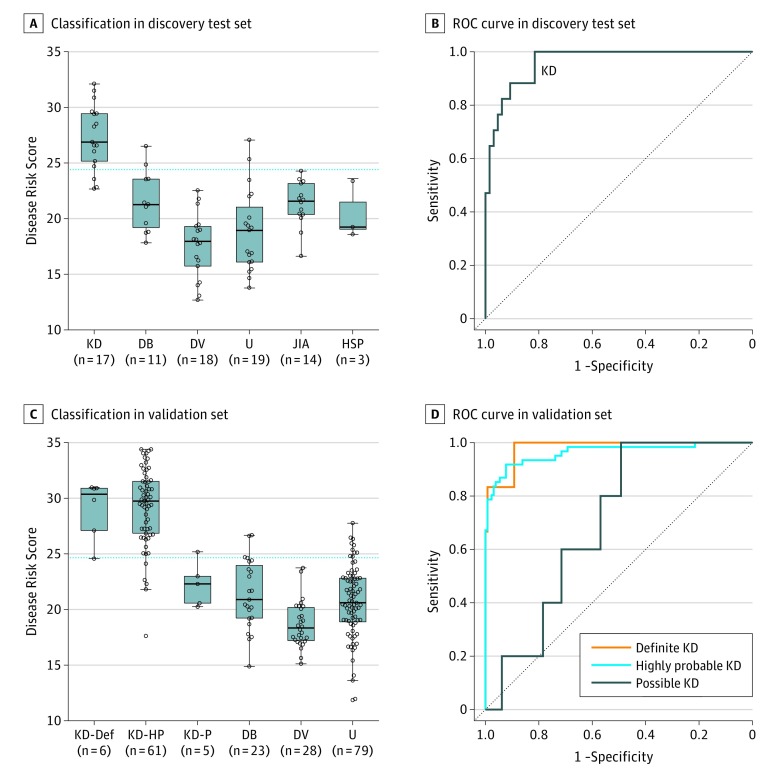
Results: Among 404 patients in the discovery set, there were 78 with KD (median age, 27 months; 55.1% male) and 326 febrile controls (median age, 37 months; 56.4% male). Among 202 patients in the validation set, there were 72 with KD (median age, 34 months; 62.5% male) and 130 febrile controls (median age, 17 months; 56.9% male). A 13-transcript signature identified in the discovery training set distinguished KD from other infectious and inflammatory conditions in the discovery test set, with AUC of 96.2% (95% CI, 92.5%-99.9%), sensitivity of 81.7% (95% CI, 60.0%-94.8%), and specificity of 92.1% (95% CI, 84.0%-97.0%). In the validation set, the signature distinguished KD from febrile controls, with AUC of 94.6% (95% CI, 91.3%-98.0%), sensitivity of 85.9% (95% CI, 76.8%-92.6%), and specificity of 89.1% (95% CI, 83.0%-93.7%). The signature was applied to clinically defined categories of definite, highly probable, and possible KD, resulting in AUCs of 98.1% (95% CI, 94.5%-100%), 96.3% (95% CI, 93.3%-99.4%), and 70.0% (95% CI, 53.4%-86.6%), respectively, mirroring certainty of clinical diagnosis.
Conclusions and relevance: In this study, a 13-transcript blood gene expression signature distinguished KD from other febrile conditions. Diagnostic accuracy increased with certainty of clinical diagnosis. A test incorporating the 13-transcript disease risk score may enable earlier diagnosis and treatment of KD and reduce inappropriate treatment in those with other diagnoses.
Conflict of interest statement
Figures
References
-
- Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974;54(3):-. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
