

Consensus on Molecular Subtypes of High-Grade Serous Ovarian Carcinoma
- PMID: 30084834
- PMCID: PMC6207081
- DOI: 10.1158/1078-0432.CCR-18-0784
Consensus on Molecular Subtypes of High-Grade Serous Ovarian Carcinoma
Abstract
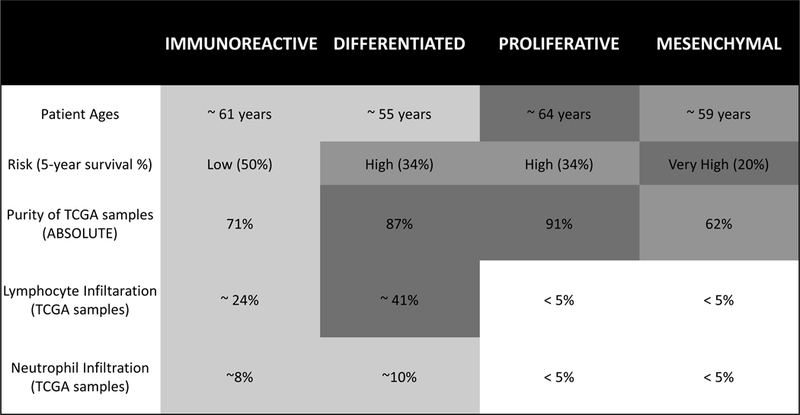
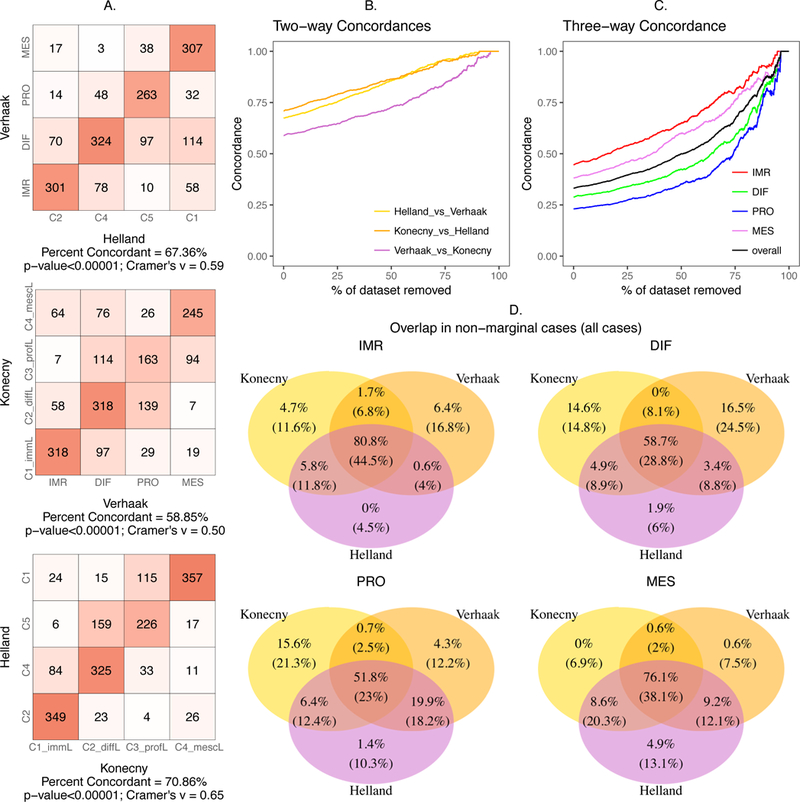
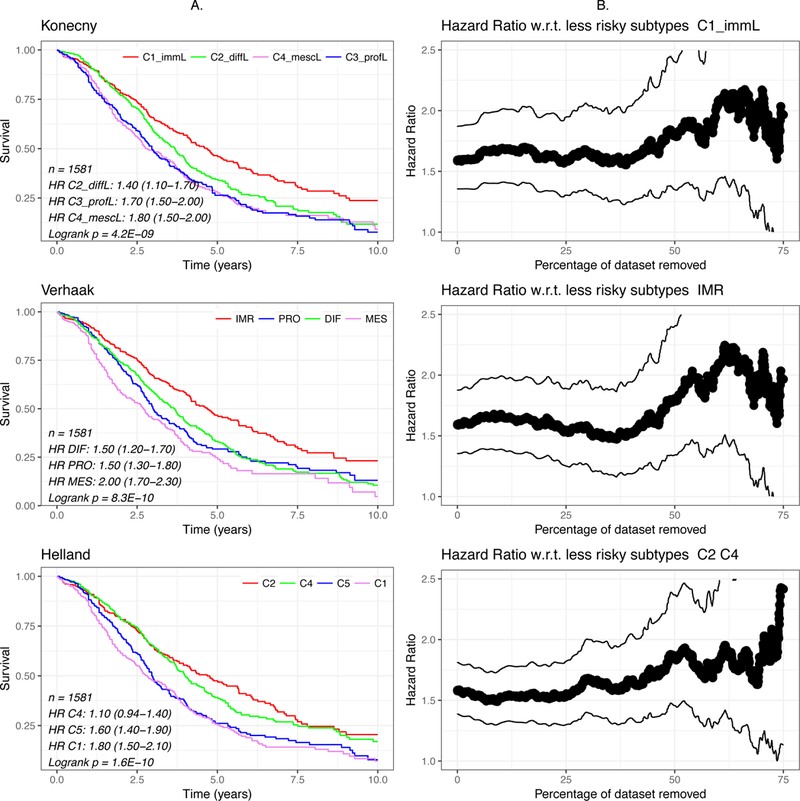
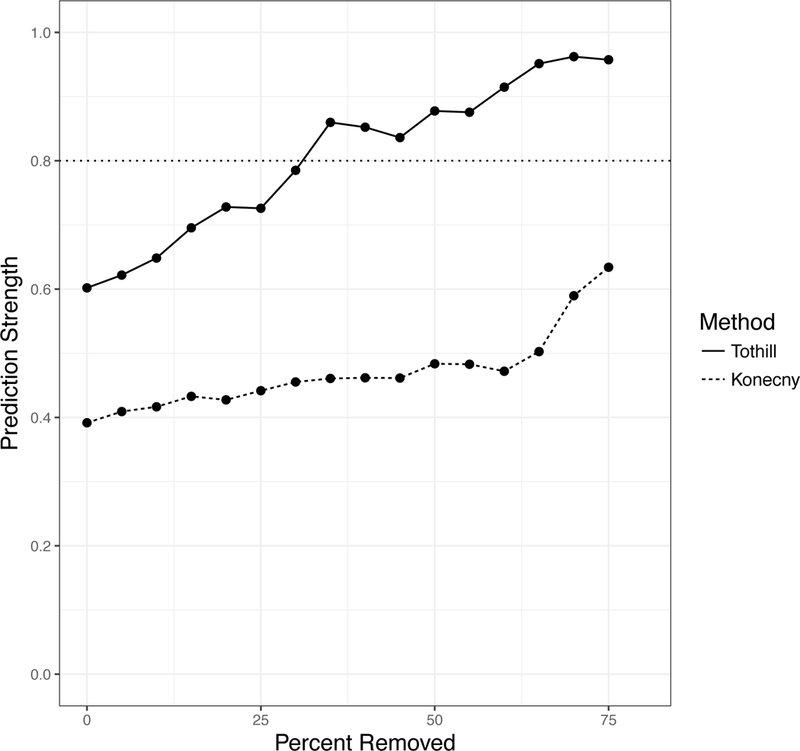
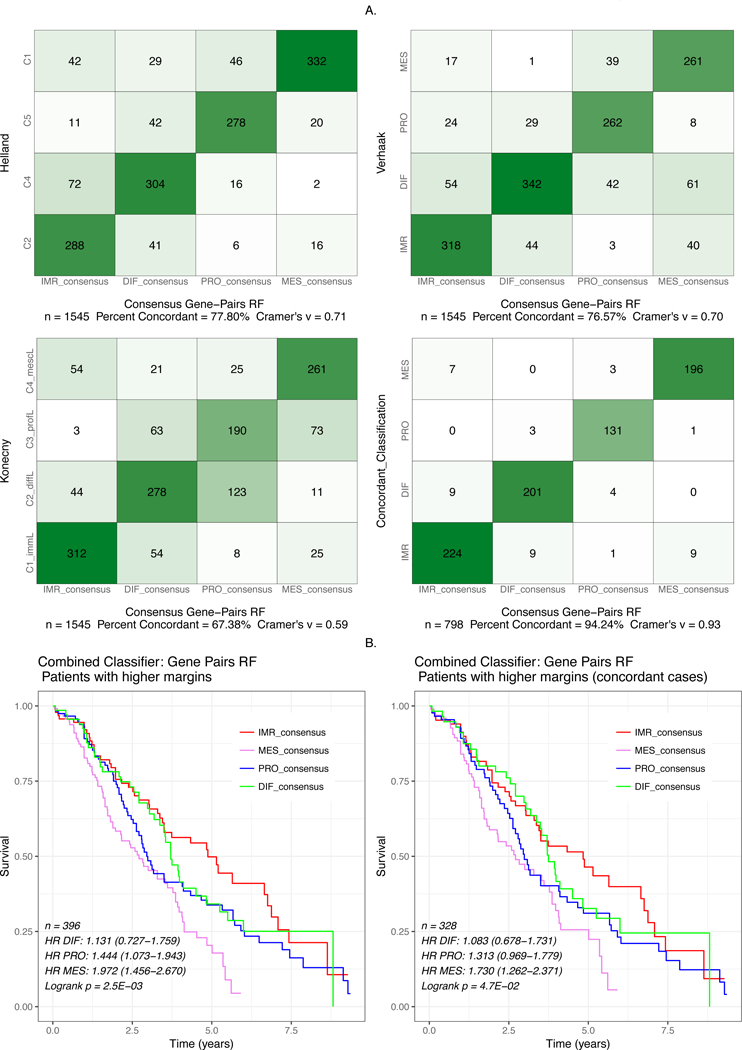
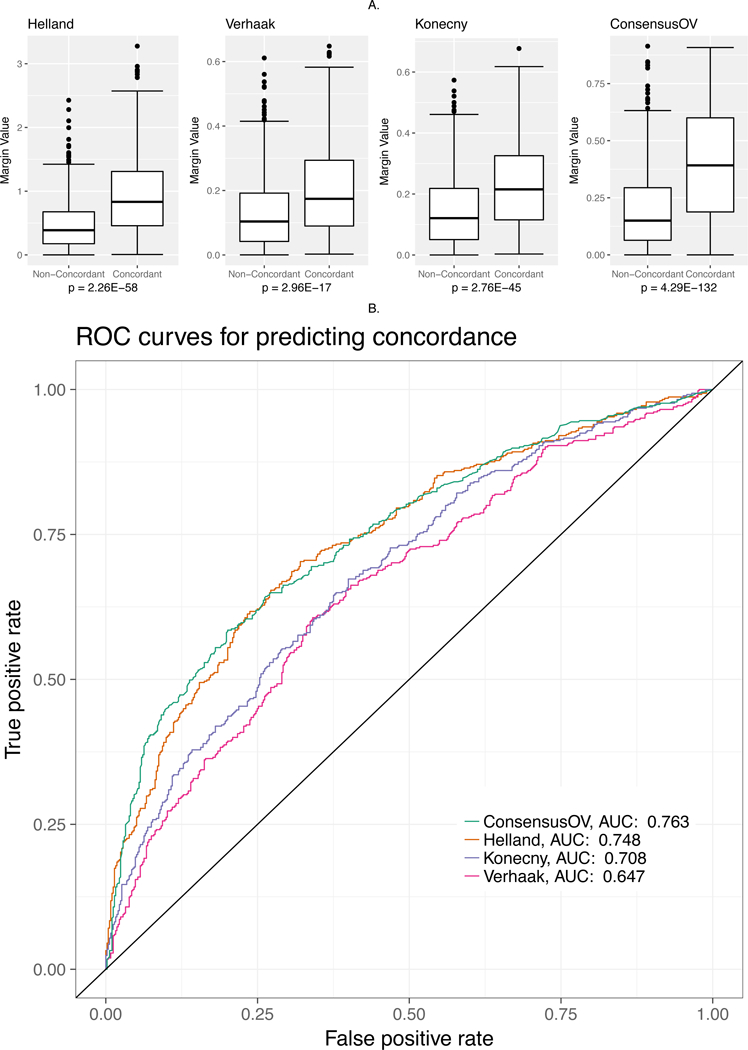
Purpose: The majority of ovarian carcinomas are of high-grade serous histology, which is associated with poor prognosis. Surgery and chemotherapy are the mainstay of treatment, and molecular characterization is necessary to lead the way to targeted therapeutic options. To this end, various computational methods for gene expression-based subtyping of high-grade serous ovarian carcinoma (HGSOC) have been proposed, but their overlap and robustness remain unknown.Experimental Design: We assess three major subtype classifiers by meta-analysis of publicly available expression data, and assess statistical criteria of subtype robustness and classifier concordance. We develop a consensus classifier that represents the subtype classifications of tumors based on the consensus of multiple methods, and outputs a confidence score. Using our compendium of expression data, we examine the possibility that a subset of tumors is unclassifiable based on currently proposed subtypes.Results: HGSOC subtyping classifiers exhibit moderate pairwise concordance across our data compendium (58.9%-70.9%; P < 10-5) and are associated with overall survival in a meta-analysis across datasets (P < 10-5). Current subtypes do not meet statistical criteria for robustness to reclustering across multiple datasets (prediction strength < 0.6). A new subtype classifier is trained on concordantly classified samples to yield a consensus classification of patient tumors that correlates with patient age, survival, tumor purity, and lymphocyte infiltration.Conclusions: A new consensus ovarian subtype classifier represents the consensus of methods and demonstrates the importance of classification approaches for cancer that do not require all tumors to be assigned to a distinct subtype. Clin Cancer Res; 24(20); 5037-47. ©2018 AACR.
©2018 American Association for Cancer Research.
Figures
References
-
- Liu J, Matulonis UA. New strategies in ovarian cancer: translating the molecular complexity of ovarian cancer into treatment advances. Clin Cancer Res. 2014;20:5150–6. - PubMed
-
- Tothill RW, Tinker AV, George J, Brown R, Fox SB, Lade S, et al. Novel molecular subtypes of serous and endometrioid ovarian cancer linked to clinical outcome. Clin Cancer Res. 2008;14:5198–208. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
