

PD-1 blockade partially recovers dysfunctional virus-specific B cells in chronic hepatitis B infection
- PMID: 30084841
- PMCID: PMC6159957
- DOI: 10.1172/JCI121957
PD-1 blockade partially recovers dysfunctional virus-specific B cells in chronic hepatitis B infection
Abstract
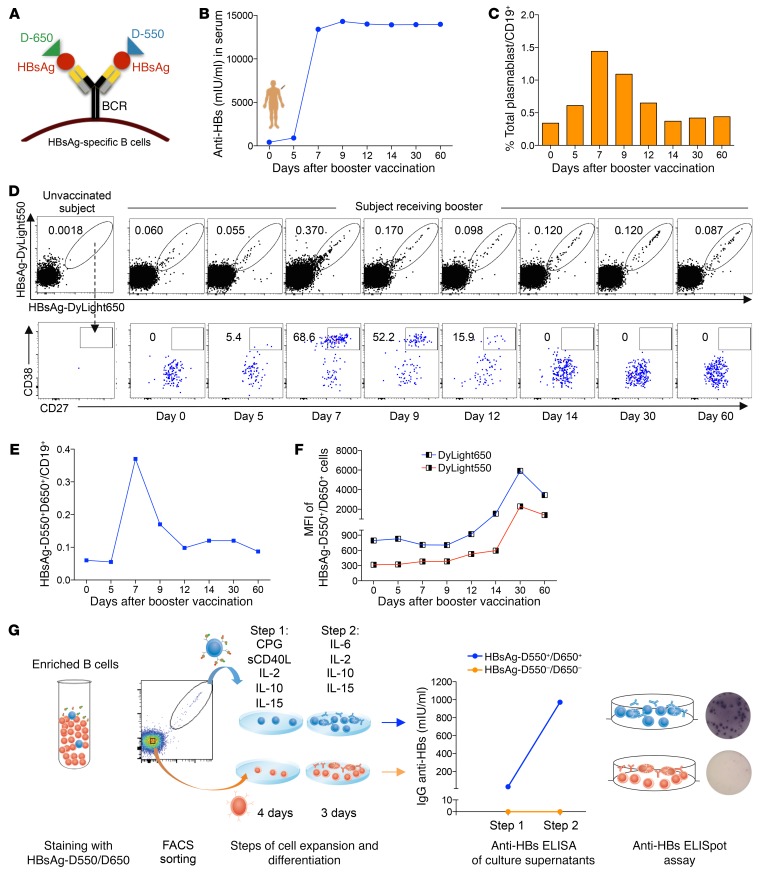
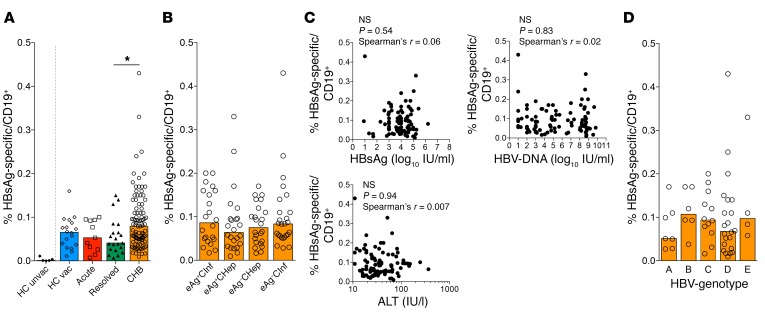
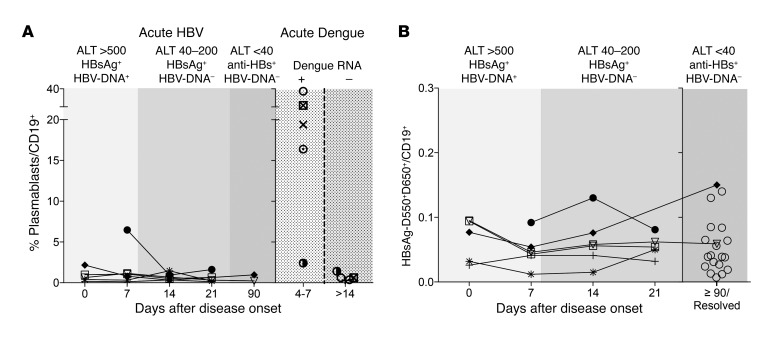
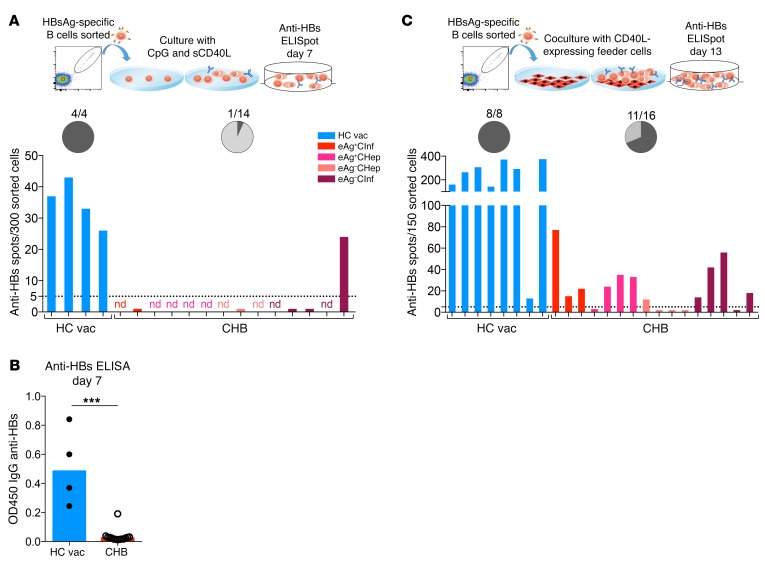
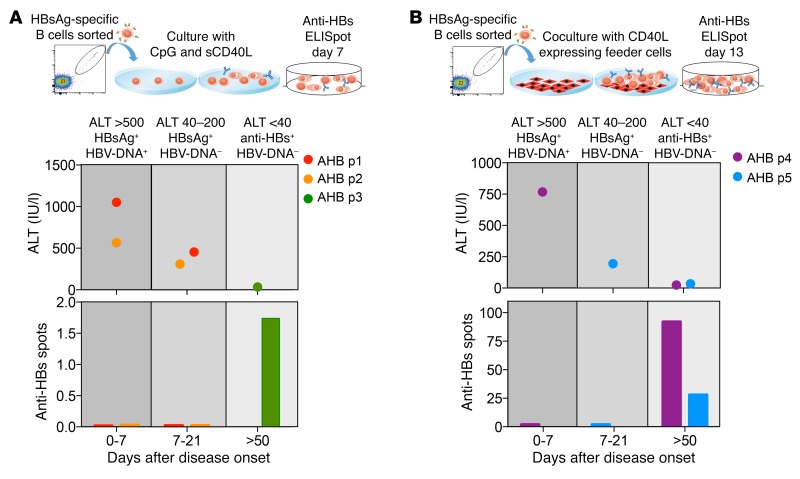
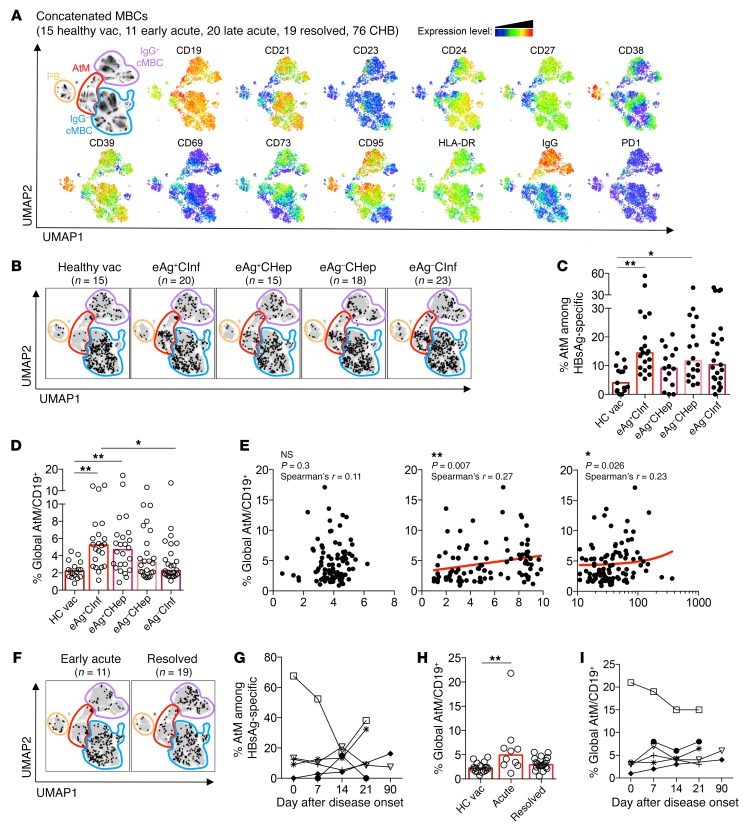
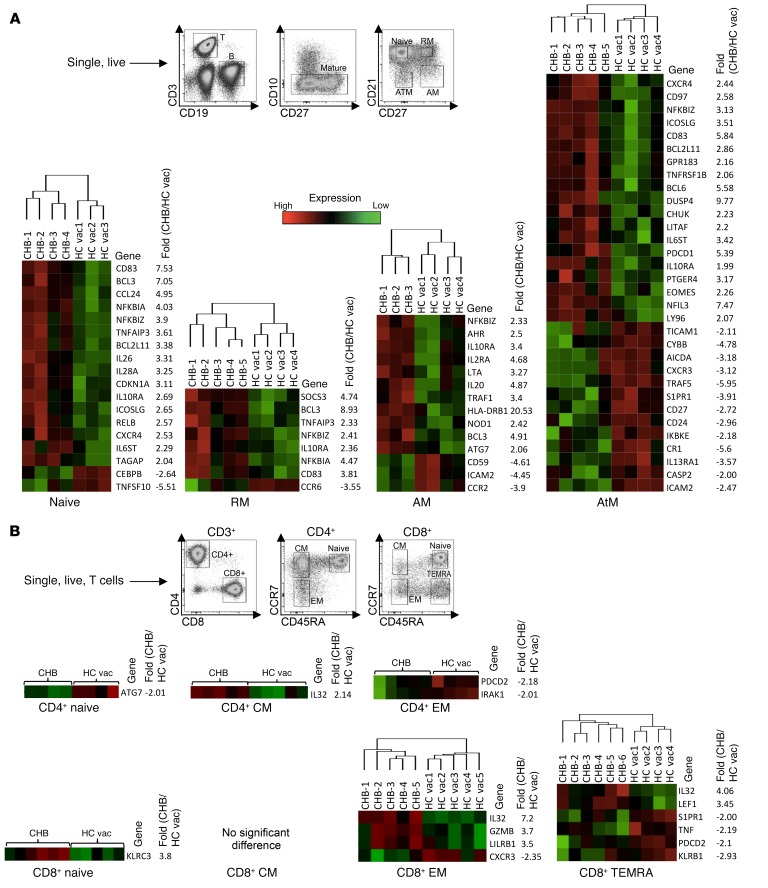
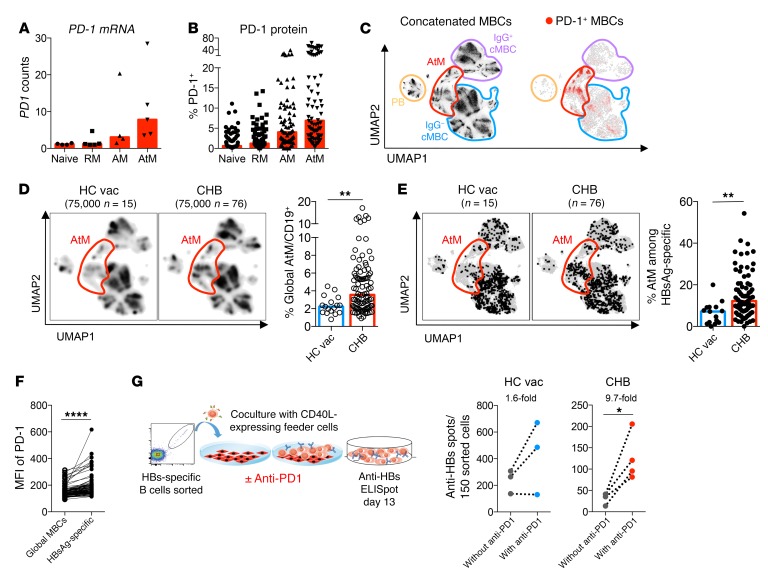
Chronic HBV (CHB) infection suppresses virus-specific T cells, but its impact on humoral immunity has been poorly analyzed. Here, we developed a dual-staining method that utilizes hepatitis B virus (HBV) surface antigens (HBsAg) labeled with fluorochromes as "baits" for specific ex vivo detection of HBsAg-specific B cells and analysis of their quantity, function, and phenotype. We studied healthy vaccinated subjects (n = 18) and patients with resolved (n = 21), acute (n = 11), or chronic (n = 96) HBV infection and observed that frequencies of circulating HBsAg-specific B cells were independent of HBV infection status. In contrast, the presence of serum HBsAg affected function and phenotype of HBsAg-specific B cells that were unable to mature in vitro into Ab-secreting cells and displayed an increased expression of markers linked to hyperactivation (CD21lo) and exhaustion (PD-1). Importantly, B cell alterations were not limited to HBsAg-specific B cells, but affected the global B cell population. HBsAg-specific B cell maturation could be partially restored by a method involving the combination of the cytokines IL-2 and IL-21 and CD40L-expressing feeder cells and was further boosted by the addition of anti-PD-1 Abs. In conclusion, HBV infection has a marked impact on global and HBV-specific humoral immunity, yet HBsAg-specific B cells are amenable to a partial rescue by B cell-maturing cytokines and PD-1 blockade.
Keywords: B cells; Hepatitis; Hepatology; Infectious disease.
Conflict of interest statement
Figures
Comment in
-
Entering the spotlight: hepatitis B surface antigen-specific B cells.J Clin Invest. 2018 Oct 1;128(10):4257-4259. doi: 10.1172/JCI124098. Epub 2018 Sep 17. J Clin Invest. 2018. PMID: 30222139 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
