

Incidence of complications related to catheter ablation of atrial fibrillation and atrial flutter: a nationwide in-hospital analysis of administrative data for Germany in 2014
- PMID: 30085086
- PMCID: PMC6269631
- DOI: 10.1093/eurheartj/ehy452
Incidence of complications related to catheter ablation of atrial fibrillation and atrial flutter: a nationwide in-hospital analysis of administrative data for Germany in 2014
Abstract
Aims: Risks of catheter ablation for atrial fibrillation and flutter assessed in retrospective studies, registries, and controlled trials may underestimate 'real world' conditions.
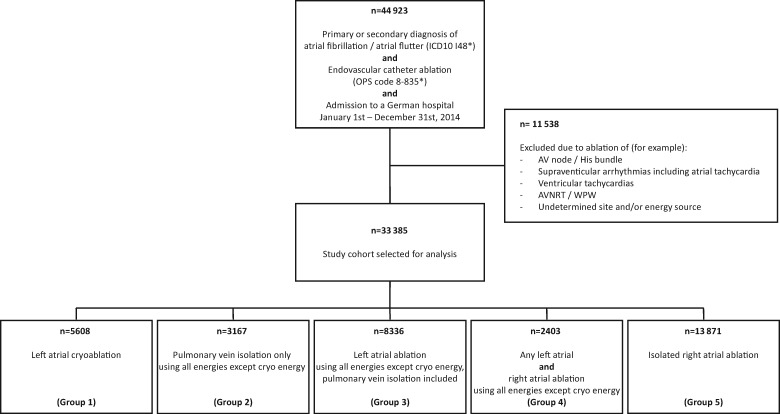
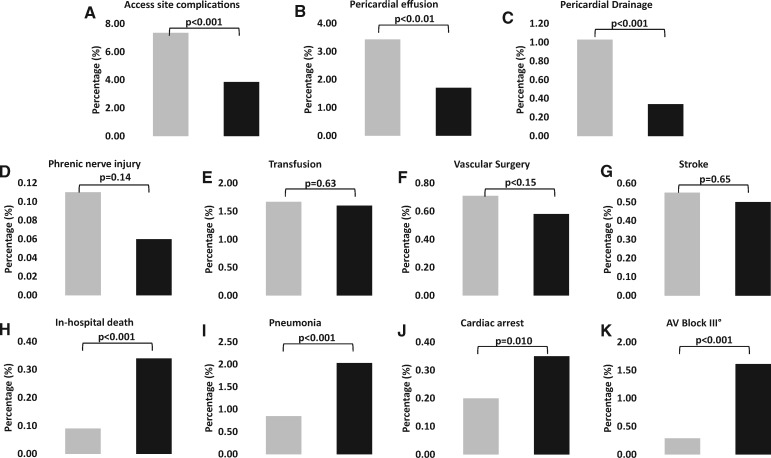
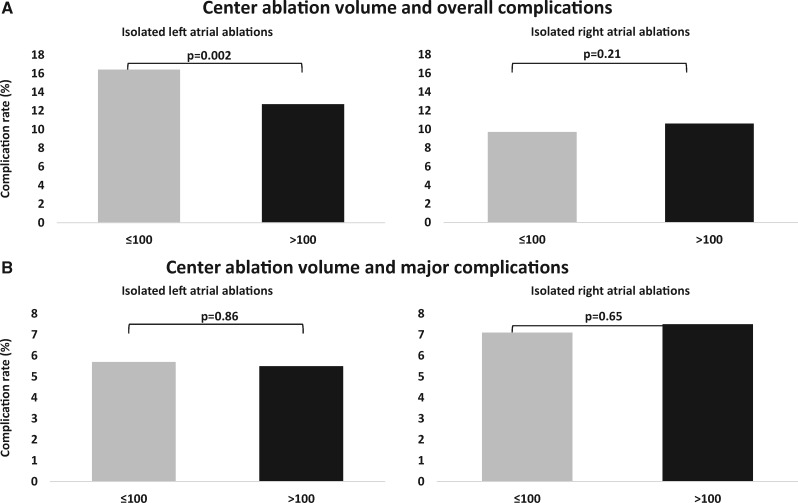
Methods and results: To assess complications in a nationwide approach, we included all cases undergoing catheter ablation for atrial fibrillation and atrial flutter in Germany in 2014, using ICD-10-GM-based German Diagnosis Related Group (G-DRG) codes and the well differentiated German Operation and Procedure Classification (OPS) analysing 33 353 in-hospital cases. For left atrial ablations (19 514 cases), the overall complication rate ranged from a mean of 11.7% to 13.8% depending on type and site of applied energy, including major complications ranging from 3.8% to 7.2%. Whereas overall complication rates were lower for atrial flutter ablations (13 871 cases, 10.5%; P < 0.001), interestingly, major complications occurred more frequently (7.4%; P < 0.001). Particularly, in-hospital death was four-times more common following right than following left atrial ablations (47 vs. 18 cases, 0.34% vs. 0.09%; P < 0.001). Stratified by centre ablation volume, significantly fewer overall complications occurred in centres performing >100 vs. ≤100 left atrial ablations annually (12.7% vs. 16.4%; P < 0.002).
Conclusion: Administrative data of all atrial fibrillation ablations in Germany in 2014 revealed higher overall and major complication rates than previously reported. Few patients were treated in low volume centres, but were exposed to a higher overall complication risk. Atrial flutter ablations were associated with surprisingly high rates of life-threatening complications. Advanced age combined with highly prevalent cardiac, pulmonary and, vascular comorbidities likely play a major role. In addition, individual-level clinical studies need to address the safety and benefits of catheter ablation in an elderly, diseased population.
Figures
References
-
- Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P, Clémenty J.. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659–666. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K.. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37:2893–2962. - PubMed
-
- Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A.. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation 2005;111:1100–1105. - PubMed
-
- Dagres N, Hindricks G, Kottkamp H, Sommer P, Gaspar T, Bode K, Arya A, Husser D, Rallidis LS, Kremastinos DT, Piorkowski C.. Complications of atrial fibrillation ablation in a high-volume center in 1,000 procedures: still cause for concern?. J Cardiovasc Electrophysiol 2009;20:1014–1019. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
