

Hypotension and a positive fluid balance are associated with delirium in patients with shock
- PMID: 30086136
- PMCID: PMC6080753
- DOI: 10.1371/journal.pone.0200495
Hypotension and a positive fluid balance are associated with delirium in patients with shock
Abstract
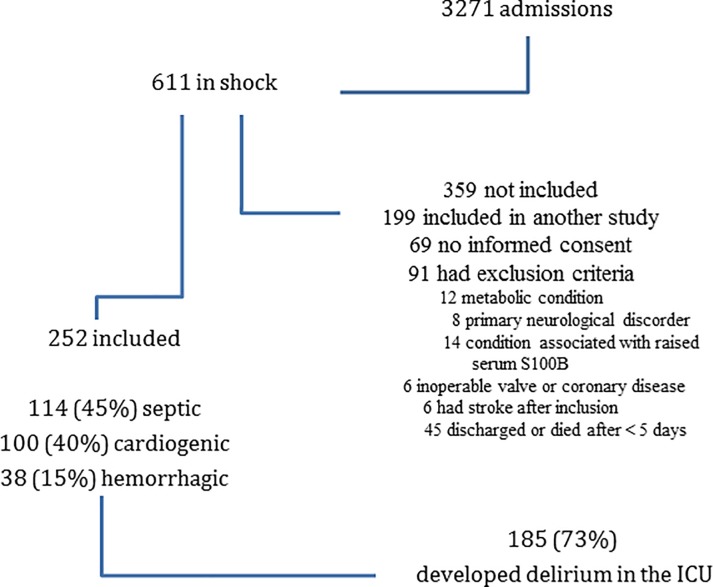
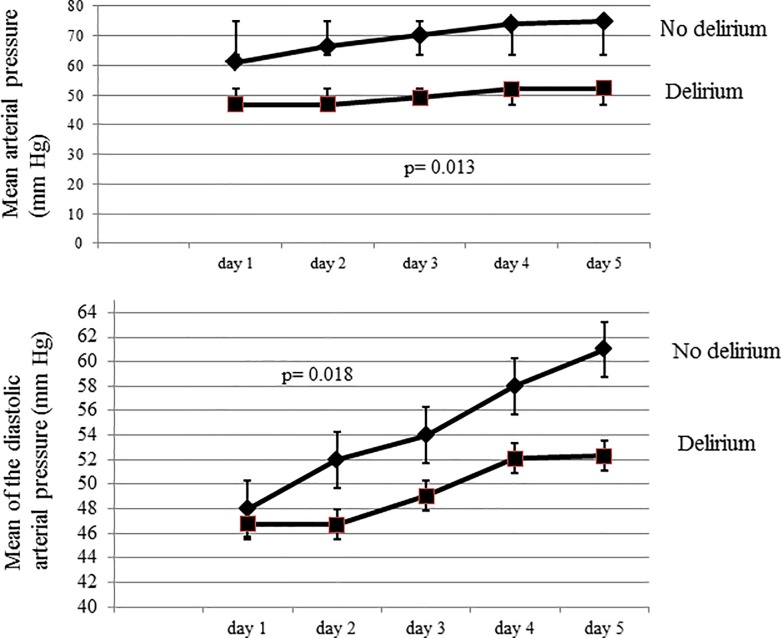
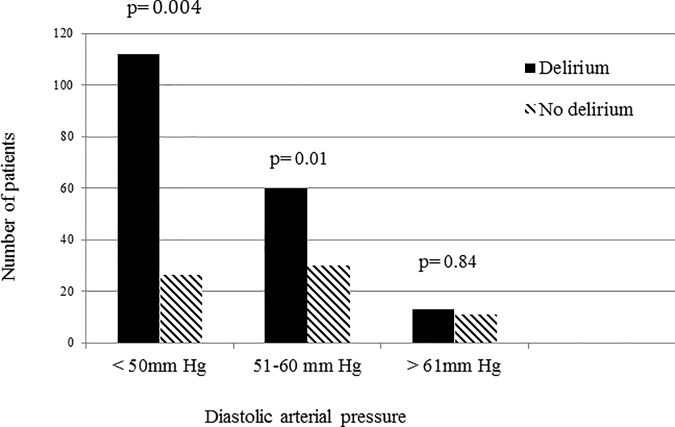
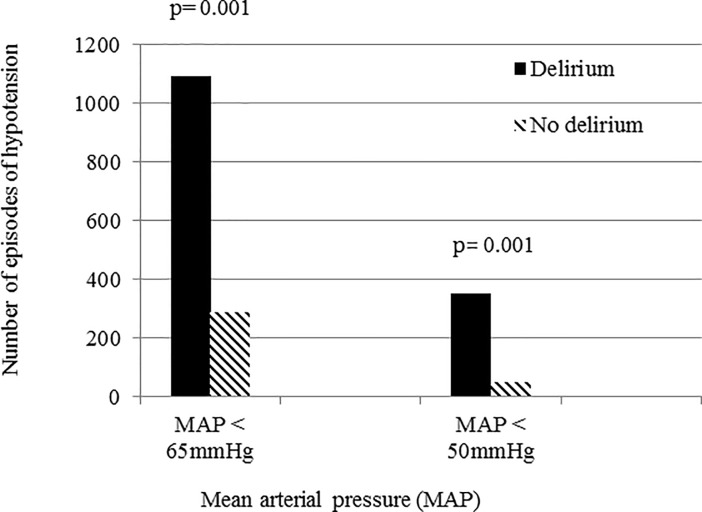
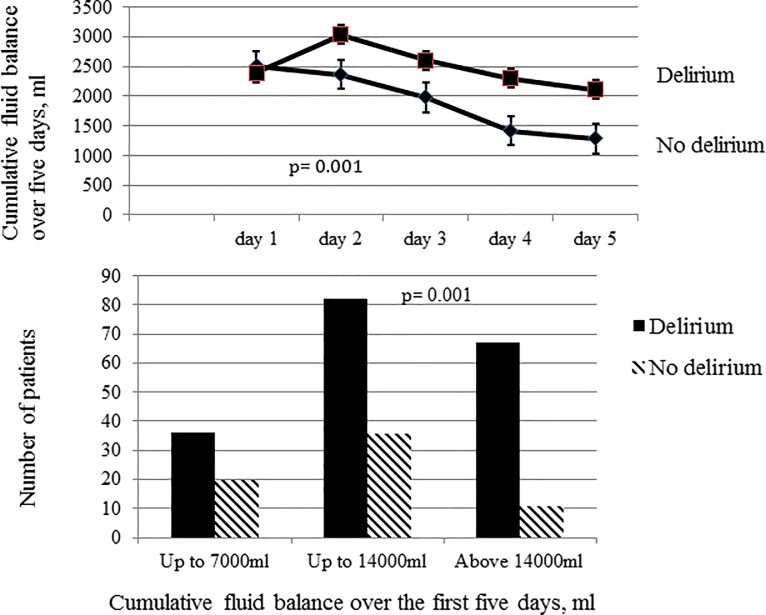
The pathogenesis of delirium in critically ill patients is multifactorial. How hypotension and hypoxemia affect brain function and whether they can promote delirium remains unclear. A high cumulative positive fluid balance may also have a negative effect on brain function and promote delirium. We hypothesized that delirium would be more likely to develop in patients with low systemic arterial pressure, hypoxemia and a higher positive fluid balance, and investigated these associations in a prospective observational cohort study in patients with shock. After initial resuscitation, episodes of hypotension, defined as a mean arterial pressure (MAP) <65 mmHg or diastolic pressure <60 mmHg, and hypoxemia, defined as peripheral oxygen saturation (SpO2) <90% for more than one minute or any arterial oxygen concentration (PaO2) <90 mmHg, were recorded during the first 5 days of the ICU stay. Fluid balance was evaluated daily and the 5-day cumulative fluid balance recorded. Delirium was assessed using the Confusion Assessment Method for the ICU. A total of 252 patients were admitted with shock during the study period; 185 (73%) developed delirium. Patients who developed delirium also had more episodes of hypotension with a low MAP (p = 0.013) or diastolic pressure (p = 0.018) during the first five days of the ICU stay than those who did not. Patients with a higher cumulative fluid balance during the same period were also more likely to develop delirium (p = 0.01); there was no significant difference in the occurrence of hypoxemia between groups. Joint modeling, combining a linear-mixed model and an adjusted Cox survival model showed that low diastolic pressure (alpha effect = -0.058±0.0013, p = 0.043) and a positive cumulative fluid balance (alpha effect = 0.04±0.003, p = 0.021) were independently associated with delirium. In conclusion, low diastolic pressure and a cumulative positive fluid balance but not hypoxemia were independently associated with development of delirium in patients with shock.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Delirium After Cardiac Surgery and Cumulative Fluid Balance: A Case-Control Cohort Study.J Cardiothorac Vasc Anesth. 2019 Jan;33(1):93-101. doi: 10.1053/j.jvca.2018.07.012. Epub 2018 Aug 17. J Cardiothorac Vasc Anesth. 2019. PMID: 30122614
-
Association Between Perioperative Hypotension and Delirium in Postoperative Critically Ill Patients: A Retrospective Cohort Analysis.Anesth Analg. 2020 Mar;130(3):636-643. doi: 10.1213/ANE.0000000000004517. Anesth Analg. 2020. PMID: 31725024
-
[Effect of global end diastolic volume index guidance fluid resuscitation in elderly patients with septic shock].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Jun;29(6):486-490. doi: 10.3760/cma.j.issn.2095-4352.2017.06.002. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 28625234 Chinese.
-
Clinical values of cerebral oxygen saturation monitoring in patients with septic shock.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021 Nov 28;46(11):1212-1219. doi: 10.11817/j.issn.1672-7347.2021.200905. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2021. PMID: 34911855 Free PMC article. Chinese, English.
-
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af. Crit Care Med. 2013. PMID: 23353941
Cited by
-
Interpretable machine learning model for predicting delirium in patients with sepsis: a study based on the MIMIC data.BMC Infect Dis. 2025 Apr 23;25(1):585. doi: 10.1186/s12879-025-10982-8. BMC Infect Dis. 2025. PMID: 40269746 Free PMC article.
-
Controlled Mechanical Ventilation in Critically Ill Patients and the Potential Role of Venous Bagging in Acute Kidney Injury.J Clin Med. 2024 Mar 5;13(5):1504. doi: 10.3390/jcm13051504. J Clin Med. 2024. PMID: 38592687 Free PMC article.
-
Hypotension during intensive care stay and mortality and morbidity: a systematic review and meta-analysis.Intensive Care Med. 2024 Apr;50(4):516-525. doi: 10.1007/s00134-023-07304-4. Epub 2024 Jan 22. Intensive Care Med. 2024. PMID: 38252288 Free PMC article.
-
Impact of a Premorbid Psychiatric Disorder on the Incidence of Delirium during ICU Stay, Morbidity, and Long-Term Mortality.Crit Care Res Pract. 2019 Jul 18;2019:6402097. doi: 10.1155/2019/6402097. eCollection 2019. Crit Care Res Pract. 2019. PMID: 31396415 Free PMC article.
-
Individual Pharmacotherapy Management (IPM) - I: a group-matched retrospective controlled clinical study on prevention of complicating delirium in the elderly trauma patients and identification of associated factors.BMC Geriatr. 2022 Jan 6;22(1):29. doi: 10.1186/s12877-021-02630-y. BMC Geriatr. 2022. PMID: 34991474 Free PMC article.
References
-
- Vincent JL, Leone M. Optimal treatment of vasopressor-dependent distributive shock. Exp Rev Anti Infect Ther 2017; 15: 5–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
