

Phosphate control in reducing FGF23 levels in hemodialysis patients
- PMID: 30086150
- PMCID: PMC6080760
- DOI: 10.1371/journal.pone.0201537
Phosphate control in reducing FGF23 levels in hemodialysis patients
Abstract
Background: In hemodialysis patients, high levels of Fibroblast Growth Factor 23 (FGF23) predict mortality. Our study was designed to test whether the control of serum phosphate is associated with a reduction in serum FGF23 levels. Additionally other variables with a potential effect on FGF23 levels were evaluated.
Material and methods: The effect of sustained (40-weeks) control of serum phosphate on FGF23 levels (intact and c-terminal) was evaluated in 21 stable hemodialysis patients that were not receiving calcimimetics or active vitamin D. Patients received non-calcium phosphate binders to maintain serum phosphate below 4.5 mg/dl. In an additional analysis, values of intact-FGF23 (iFGF23) and c-terminal FGF23 (cFGF23) from 150 hemodialysis patients were correlated with parameters of mineral metabolism and inflammation. Linear mixed models and linear regression were performed to evaluate longitudinal trajectories of variables and the association between FGF23 and the other variables examined.
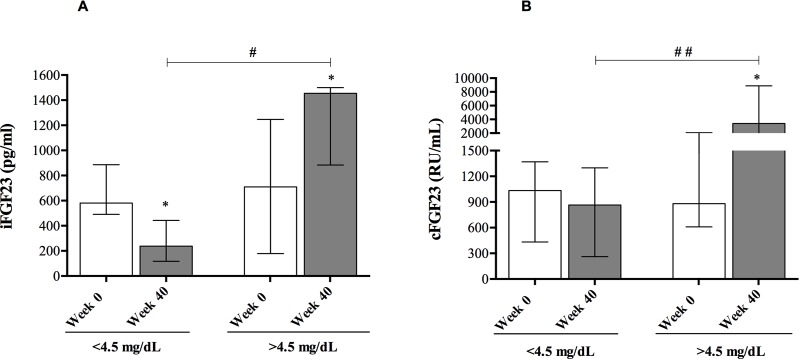
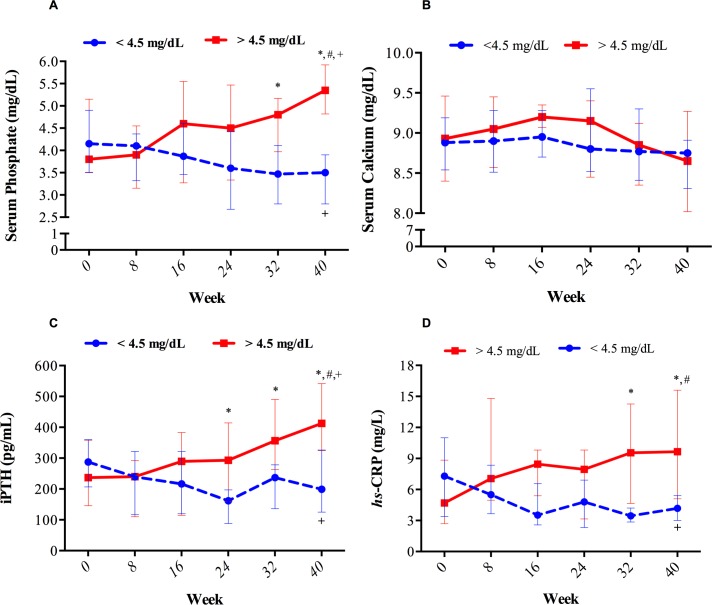
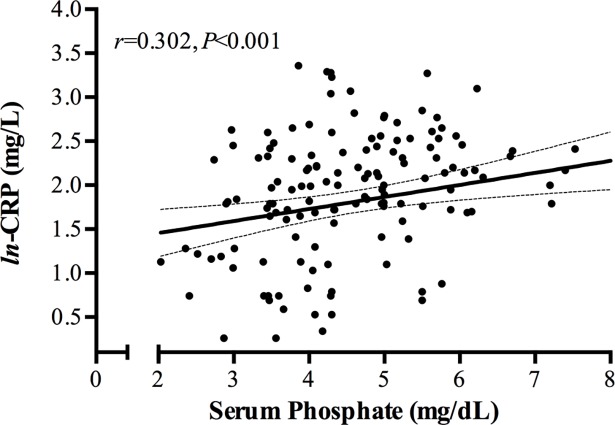
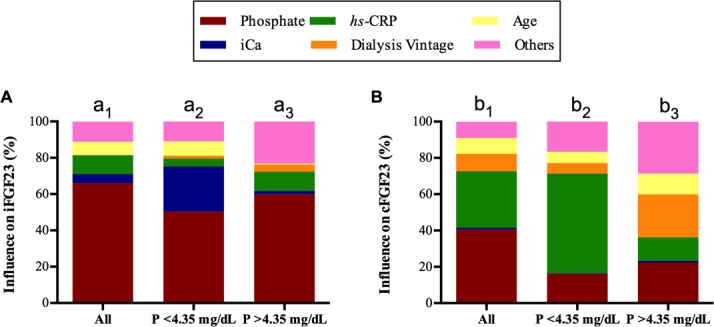
Results: During the 40-week treatment, 12 of 21 patients achieved the target of serum phosphate <4.5 mg/dl. In these 12 patients, iFGF23 decreased to less than half whereas cFGF23 did not reduce significantly. In patients with serum phosphate >4.5 mg, iFGF23 and cFGF23 increased two and four-fold respectively as compared with baseline. Furthermore, changes in serum phosphate correlated with changes in C-reactive protein (hs-CRP). In our 150 hemodialysis patients, those in the higher tertile of serum phosphate also showed increased hs-CRP, iPTH, iFGF23 and cFGF23. Multiple regression analysis revealed that iFGF23 levels directly correlated with both serum phosphate and calcium, whereas cFGF23 correlated with serum phosphate and hs-CRP but not with calcium.
Conclusions: The control of serum phosphate reduced iFGF23. This reduction was also associated with a decreased in inflammatory parameters. Considering the entire cohort of hemodialysis patients, iFGF23 levels correlated directly with serum phosphate levels and also correlated inversely with serum calcium concentration. The levels of cFGF23 were closely related to serum phosphate and parameters of inflammation.
Conflict of interest statement
MAAL has received lecture fees from Fresenius Medical Care and AMGEN. M.R. has received research grants from Amgen and Fresenius Medical Care and lecture fees from the following companies: Amgen, Abbott, Shire, and Fresenius Medical Care. AMM has received lecture fees from Fresenius Medical Care and Bellco in the last two years. All the other authors declare no conflict of interest to disclose. The companies pointed in the financial disclosures had no role in the study design, collection, analysis, interpretation of data nor preparation of the manuscript. The results presented in this paper have not been published previously in whole or part, except in abstract format. This does not alter our adherence to PLOS ONE policies on sharing data and materials
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
