

Facilitated expansion of Th17 cells in lupus nephritis patients
- PMID: 30086206
- PMCID: PMC6230997
- DOI: 10.1111/cei.13196
Facilitated expansion of Th17 cells in lupus nephritis patients
Abstract
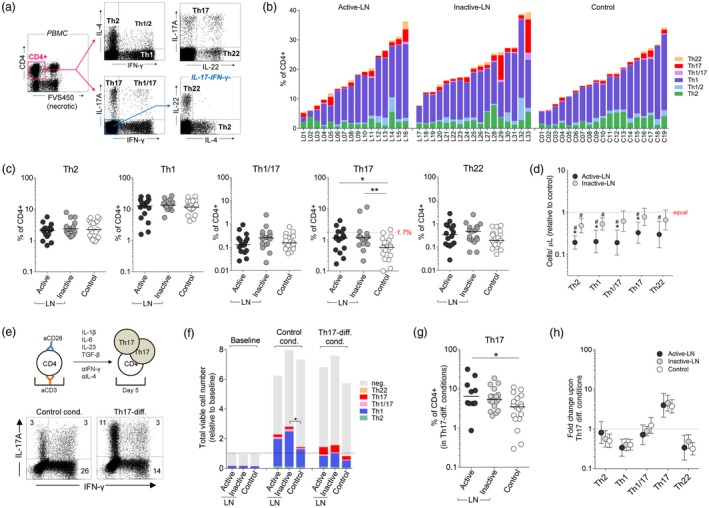
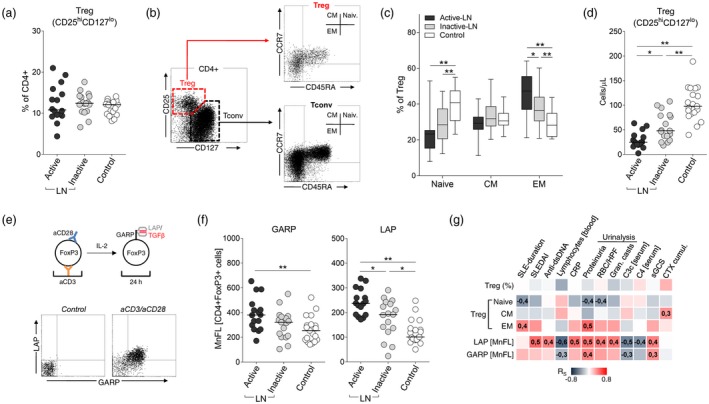
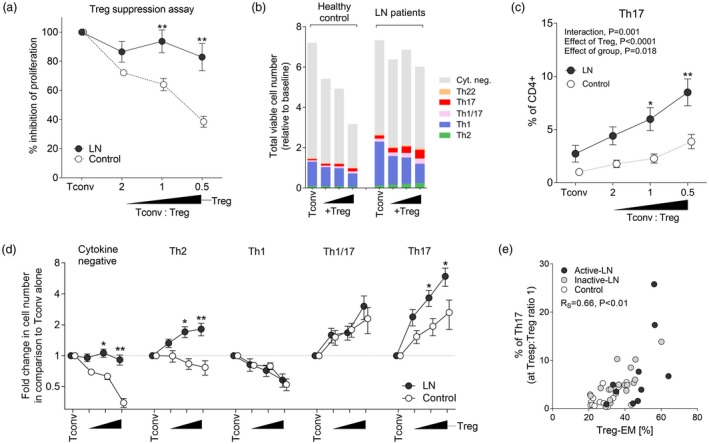
The objective of this study was to investigate the mechanisms of T helper type 17 (Th17) expansion in lupus nephritis (LN) patients, and to determine whether or not it is associated with impaired function of regulatory T cells (Treg ). Major effector subsets of peripheral blood CD4+ T cells were assessed by flow cytometry in 33 LN patients with different activity of the disease and 19 healthy controls. The percentage of circulating Th17 cells was increased in LN (median = 1·2% of CD4+ compared to 0·6% in the control group, P < 0·01), while Treg cells remained unchanged (12·3 versus 12·1% in controls), resulting in a significantly lower Treg /Th17 ratio. Th17 expansion in the patient group was not related to LN activity, renal histology or blood and urine inflammatory biomarkers, but has been associated with a higher cumulative dose of cyclophosphamide. Treg cells in LN displayed mainly effector memory phenotype and expressed higher levels of transforming growth factor (TGF)-β; however, their suppressant activity in lymphocyte proliferation assay was diminished compared to controls (~fourfold, P < 0·05). Co-culture of Treg and conventional CD4+ T cells resulted in marked suppression of the Th1 subset in both of the groups studied, but also in a potent expansion of Th17 cells, which in LN was twofold higher, as in controls (P < 0·05). In conclusion, our results demonstrate that Th17 expansion in LN is not increased during disease exacerbation, but is related to chronic immunosuppressive therapy. This immune signature is probably linked to the abnormal function of Treg cells, which were less suppressive in LN patients and even facilitated differentiation of Th17 cells.
Keywords: Th17 cells; lupus nephritis; regulatory T cells; systemic lupus erythematosus.
© 2018 British Society for Immunology.
Figures
References
-
- Kaul A, Gordon C, Crow MK et al. Systemic lupus erythematosus. Nat Rev Dis Primers 2016;2:16039. - PubMed
-
- Borchers AT, Leibushor N, Naguwa SM, Cheema GS, Shoenfeld Y, Gershwin ME. Lupus nephritis: a critical review. Autoimmun Rev 2012;12:174–94. - PubMed
-
- Krebs CF, Schmidt T, Riedel JH, Panzer U. T helper type 17 cells in immune‐mediated glomerular disease. Nat Rev Nephrol 2017;13:647–59. - PubMed
-
- Hemdan NY, Birkenmeier G, Wichmann G, Abu El‐Saad AM, Krieger T, Conrad K, Sack U. Interleukin‐17‐producing T helper cells in autoimmunity. Autoimmun Rev 2010;9:785–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
