

Transcriptomic signatures reveal immune dysregulation in human diabetic and idiopathic gastroparesis
- PMID: 30086735
- PMCID: PMC6081936
- DOI: 10.1186/s12920-018-0379-1
Transcriptomic signatures reveal immune dysregulation in human diabetic and idiopathic gastroparesis
Abstract
Background: Cellular changes described in human gastroparesis have revealed a role for immune dysregulation, however, a mechanistic understanding of human gastroparesis and the signaling pathways involved are still unclear.
Methods: Diabetic gastroparetics, diabetic non-gastroparetic controls, idiopathic gastroparetics and non-diabetic non-gastroparetic controls underwent full-thickness gastric body biopsies. Deep RNA sequencing was performed and pathway analysis of differentially expressed transcripts was done using Ingenuity®. A subset of differentially expressed genes in diabetic gastroparesis was validated in a separate cohort using QT-PCR.
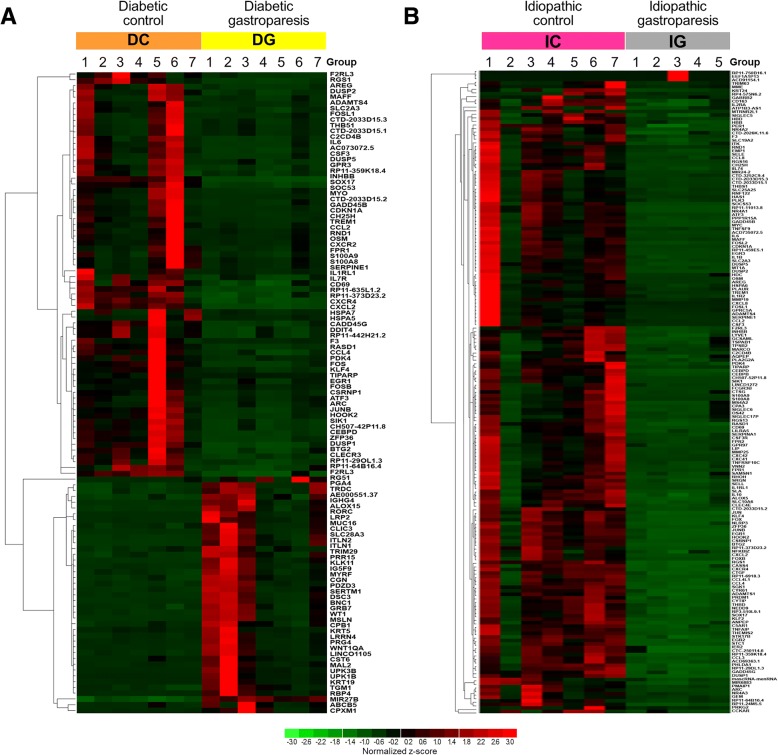
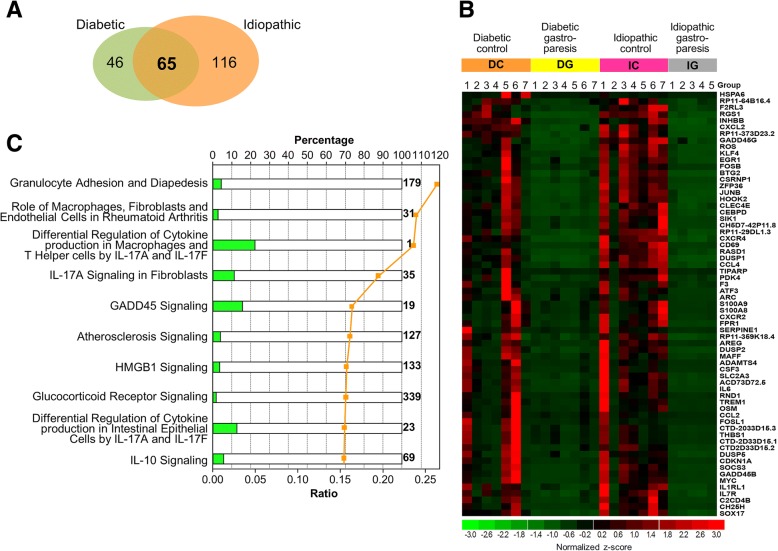
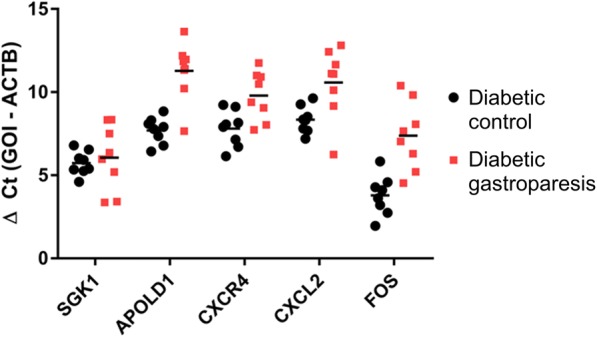
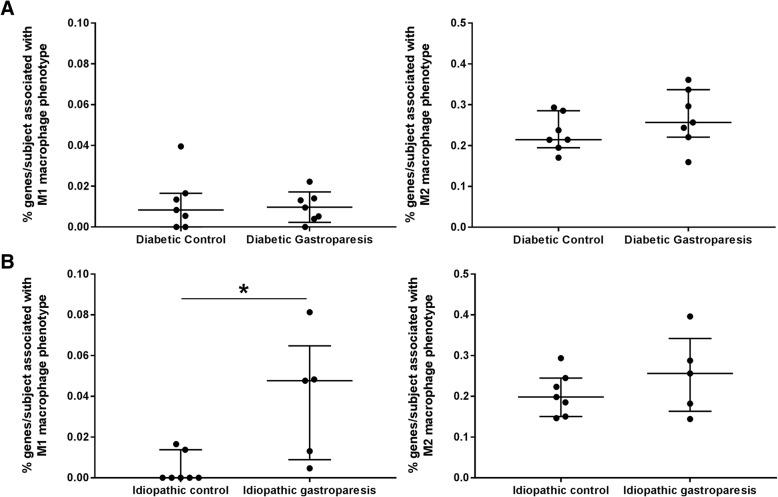
Results: 111 genes were differentially expressed in diabetic gastroparesis and 181 in idiopathic gastroparesis with a log2fold difference of | ≥ 2| and false detection rate (FDR) < 5%. Top canonical pathways in diabetic gastroparesis included genes involved with macrophages, fibroblasts and endothelial cells in rheumatoid arthritis, osteoarthritis pathway and differential regulation of cytokine production in macrophages and T helper cells by IL-17A and IL-17F. Top canonical pathways in idiopathic gastroparesis included genes involved in granulocyte adhesion and diapedesis, agranulocyte adhesion and diapedesis, and role of macrophages, fibroblasts and endothelial cells in rheumatoid arthritis. Sixty-five differentially expressed genes (log2fold difference | ≥ 2|, FDR < 5%) were common in both diabetic and idiopathic gastroparesis with genes in the top 5 canonical pathways associated with immune signaling. 4/5 highly differentially expressed genes (SGK1, APOLD1, CXCR4, CXCL2, and FOS) in diabetic gastroparesis were validated in a separate cohort of patients using RT-PCR. Immune profile analysis revealed that genes associated with M1 (pro inflammatory) macrophages were enriched in tissues from idiopathic gastroparesis tissues compared to controls (p < 0.05).
Conclusions: Diabetic and idiopathic gastroparesis have both unique and overlapping transcriptomic signatures. Innate immune signaling likely plays a central role in pathogenesis of human gastroparesis.
Keywords: Diabetes mellitus; Macrophages; Next generation sequencing; RNA; Signaling.
Conflict of interest statement
Ethics approval and consent to participate
IRB approval obtained at all clinical sites and at Mayo Clinic as follows: Temple University Office for Human Subjects Protections (FWA00004964); California Pacific Medical Center Research Institute (FWA00000921); Texas Tech University Health Sciences Center (El Paso) (FWA 00006767); University of Mississippi Medical Center (FWA00003630) and Mayo Clinic (IRB 07–003371). Written informed consent was obtained for gastroparesis cases and verbal consent was obtained for controls as per approval by respective IRBs.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Grover M, Bernard CE, Pasricha PJ, Lurken MS, Faussone-Pellegrini MS, Smyrk TC, et al. Clinical-histological associations in gastroparesis: results from the gastroparesis clinical research consortium. Neurogastroenterol Motil. 2012;24(6):531–539. doi: 10.1111/j.1365-2982.2012.01894.x. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- U24 DK074008/DK/NIDDK NIH HHS/United States
- U01 DK074008/DK/NIDDK NIH HHS/United States
- K23DK103911/DK/NIDDK NIH HHS/United States
- U01 DK112194/DK/NIDDK NIH HHS/United States
- U01DK074007/DK/NIDDK NIH HHS/United States
- U01 DK073975/DK/NIDDK NIH HHS/United States
- K23 DK103911/DK/NIDDK NIH HHS/United States
- U01DK073974/DK/NIDDK NIH HHS/United States
- P01 DK068055/DK/NIDDK NIH HHS/United States
- U01 DK074007/DK/NIDDK NIH HHS/United States
- U01DK073975/DK/NIDDK NIH HHS/United States
- U01 DK073974/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
