

Associations and prognostic significance of diffuse myocardial fibrosis by cardiovascular magnetic resonance in heart failure with preserved ejection fraction
- PMID: 30086783
- PMCID: PMC6081897
- DOI: 10.1186/s12968-018-0477-4
Associations and prognostic significance of diffuse myocardial fibrosis by cardiovascular magnetic resonance in heart failure with preserved ejection fraction
Abstract
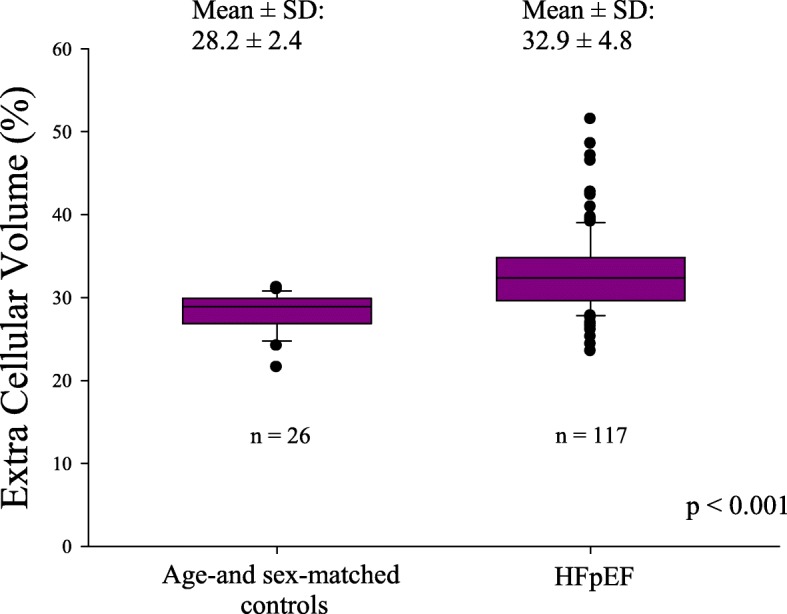
Background: Increased myocardial fibrosis may play a key role in heart failure with preserved ejection fraction (HFpEF) pathophysiology. The study aim was to evaluate the presence, associations, and prognostic significance of diffuse fibrosis in HFpEF patients compared to age- and sex-matched controls.
Methods: We prospectively included 118 consecutive HFpEF patients. Diffuse myocardial fibrosis was estimated by extracellular volume (ECV) quantified by cardiovascular magnetic resonance with the modified Look-Locker inversion recovery sequence. We determined an ECV age- and sex-adjusted cutoff value (33%) in 26 controls.
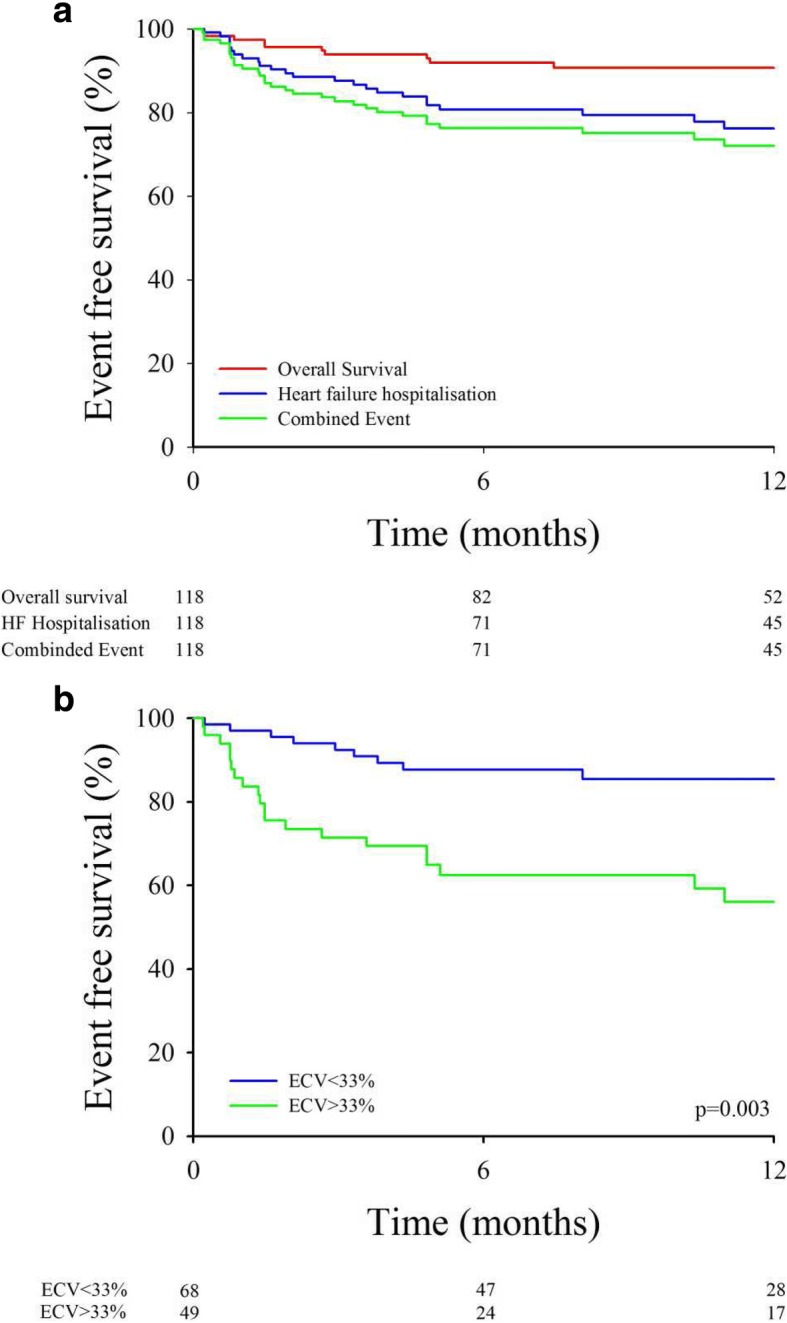
Results: Mean ECV was significantly higher in HFpEF patients versus healthy controls (32.9 ± 4.8% vs 28.2 ± 2.4%, P < 0.001). Multivariate logistic regression showed that body mass index (BMI) (odds ratio (OR) =0.92 [0.86-0.98], P = 0.011), diabetes (OR = 2.62 [1.11-6.18], P = 0.028), and transmitral peak E wave velocity (OR = 1.02 [1.00-1.03], P = 0.022) were significantly associated with abnormal ECV value. During a median follow-up of 11 ± 6 months, the primary outcome (all-cause mortality or first heart failure hospitalization) occurred in 38 patients. In multivariate Cox regression analysis, diabetes (hazard ratio (HR) =1.98 [1.04; 3.76], P = 0.038) and hemoglobin level (HR = 0.81 [0.67; 0.98], P = 0.028) were significant predictors of composite outcome. The ECV ability to improve this model added significant prognostic information. We then developed a risk score including diabetes, hemoglobin and ECV > 33% demonstrating significant prediction of risk and validated this score in a validation cohort of 53 patients. Kaplan-Meier curves showed a significant difference according to tertiles of the probability score (P < 0.001).
Conclusion: Among HFpEF patients, high ECV, likely reflecting abnormal diffuse myocardial fibrosis, was associated with a higher rate of all-cause death and first HF hospitalization in short term follow up.
Trial registration: Characterization of Heart Failure With Preserved Ejection Fraction.
Trial registration number: NCT03197350 . Date of registration: 20/06/2017. This trial was retrospectively registered.
Keywords: Cardiac magnetic resonance; Diffuse myocardial fibrosis; Prognosis.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the IRB of the Cliniques St. Luc, Université Catholique de Louvain and all participants gave written permission to participating in the study.
Consent for publication
NA
Competing interests
The Cliniques St. Luc UCL has a master clinical research agreement with Philips Medical Instruments, and the MOLLI patch was supplied by Philips Healthcare under the terms of this agreement. The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, Hernandez AF, Fonarow GC. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation. 2012;126:65–75. doi: 10.1161/CIRCULATIONAHA.111.080770. - DOI - PubMed
-
- Mohammed SF, Borlaug BA, Roger VL, Mirzoyev SA, Rodeheffer RJ, Chirinos JA, Redfield MM. Comorbidity and ventricular and vascular structure and function in heart failure with preserved ejection fraction: a community-based study. Circ Heart Fail. 2012;5:710–719. doi: 10.1161/CIRCHEARTFAILURE.112.968594. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
