

Statin as a novel pharmacotherapy of pulmonary alveolar proteinosis
- PMID: 30087322
- PMCID: PMC6081448
- DOI: 10.1038/s41467-018-05491-z
Statin as a novel pharmacotherapy of pulmonary alveolar proteinosis
Abstract
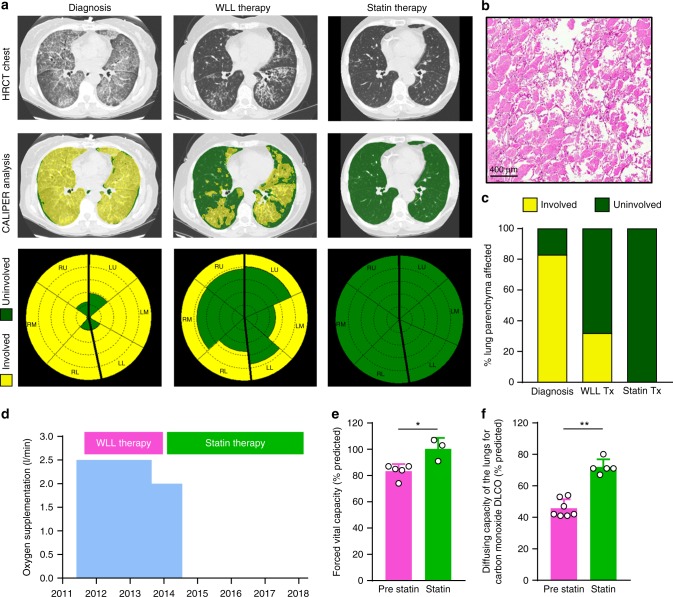
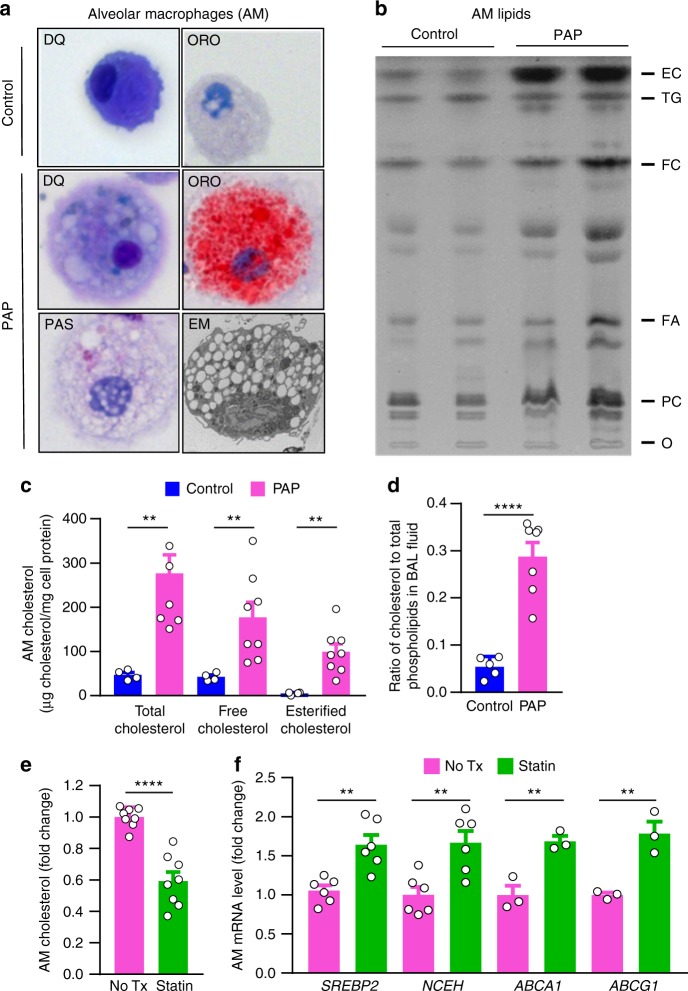
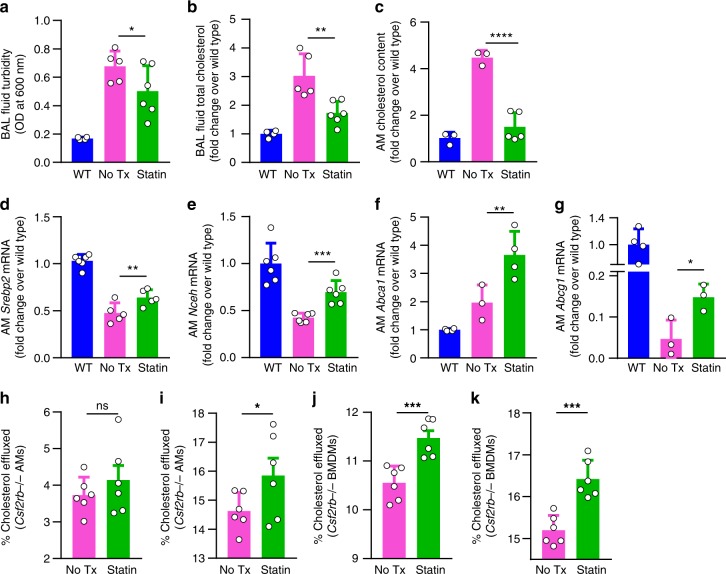
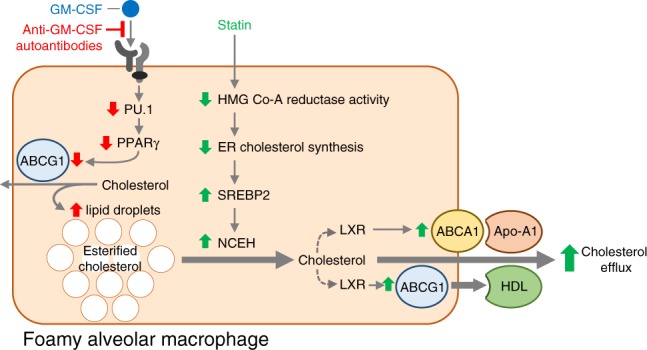
Pulmonary alveolar proteinosis (PAP) is a syndrome of reduced GM-CSF-dependent, macrophage-mediated surfactant clearance, dysfunctional foamy alveolar macrophages, alveolar surfactant accumulation, and hypoxemic respiratory failure for which the pathogenetic mechanism is unknown. Here, we examine the lipids accumulating in alveolar macrophages and surfactant to define the pathogenesis of PAP and evaluate a novel pharmacotherapeutic approach. In PAP patients, alveolar macrophages have a marked increase in cholesterol but only a minor increase in phospholipids, and pulmonary surfactant has an increase in the ratio of cholesterol to phospholipids. Oral statin therapy is associated with clinical, physiological, and radiological improvement in autoimmune PAP patients, and ex vivo statin treatment reduces cholesterol levels in explanted alveolar macrophages. In Csf2rb-/- mice, statin therapy reduces cholesterol accumulation in alveolar macrophages and ameliorates PAP, and ex vivo statin treatment increases cholesterol efflux from macrophages. These results support the feasibility of statin as a novel pathogenesis-based pharmacotherapy of PAP.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Emerging Medical Therapies for Pulmonary Alveolar Proteinosis.Am J Respir Crit Care Med. 2021 Jun 15;203(12):1566-1568. doi: 10.1164/rccm.202011-4260RR. Am J Respir Crit Care Med. 2021. PMID: 33891826 No abstract available.
References
-
- Perez-Gil J, Weaver TE. Pulmonary surfactant pathophysiology: current models and open questions. Physiol. (Bethesda). 2010;25:132–141. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL1085453/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)/International
- R01 HL136543/HL/NHLBI NIH HHS/United States
- HL118161/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)/International
- R01 HL085453/HL/NHLBI NIH HHS/United States
- R01 HL131634/HL/NHLBI NIH HHS/United States
- HL127672/U.S. Department of Health & Human Services | NIH | National Center for Advancing Translational Sciences (NCATS)/International
- R01 HL118342/HL/NHLBI NIH HHS/United States
- U54 HL127672/HL/NHLBI NIH HHS/United States
- HL136543/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)/International
- R01 HL136721/HL/NHLBI NIH HHS/United States
- R00 HL118161/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
