

Labor Induction versus Expectant Management in Low-Risk Nulliparous Women
- PMID: 30089070
- PMCID: PMC6186292
- DOI: 10.1056/NEJMoa1800566
Labor Induction versus Expectant Management in Low-Risk Nulliparous Women
Abstract
Background: The perinatal and maternal consequences of induction of labor at 39 weeks among low-risk nulliparous women are uncertain.
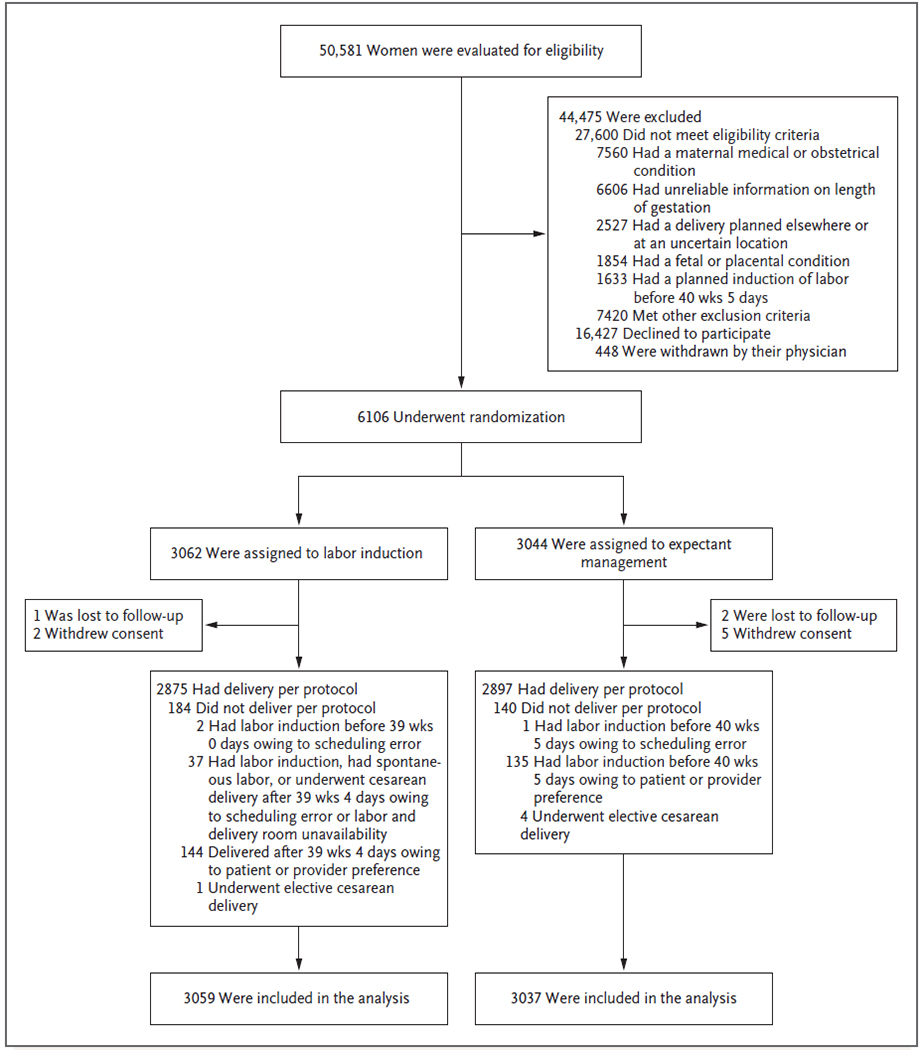
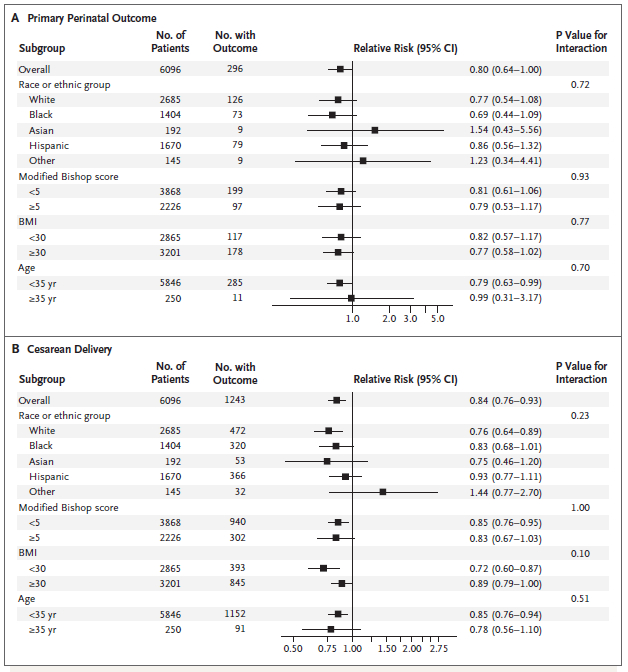
Methods: In this multicenter trial, we randomly assigned low-risk nulliparous women who were at 38 weeks 0 days to 38 weeks 6 days of gestation to labor induction at 39 weeks 0 days to 39 weeks 4 days or to expectant management. The primary outcome was a composite of perinatal death or severe neonatal complications; the principal secondary outcome was cesarean delivery.
Results: A total of 3062 women were assigned to labor induction, and 3044 were assigned to expectant management. The primary outcome occurred in 4.3% of neonates in the induction group and in 5.4% in the expectant-management group (relative risk, 0.80; 95% confidence interval [CI], 0.64 to 1.00). The frequency of cesarean delivery was significantly lower in the induction group than in the expectant-management group (18.6% vs. 22.2%; relative risk, 0.84; 95% CI, 0.76 to 0.93).
Conclusions: Induction of labor at 39 weeks in low-risk nulliparous women did not result in a significantly lower frequency of a composite adverse perinatal outcome, but it did result in a significantly lower frequency of cesarean delivery. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; ARRIVE ClinicalTrials.gov number, NCT01990612 .).
Conflict of interest statement
Dr. Silver reports receiving consulting fees from Gestavision. No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- American College of Obstetricians and Gynecologists. Practice bulletin no. 146: management of late-term and postterm pregnancies. Obstet Gynecol 2014; 124: 390–6. - PubMed
-
- ACOG Committee on Practice Bulletins — Obstetrics. ACOG practice bulletin no. 107: induction of labor. Obstet Gynecol 2009; 114: 386–97. - PubMed
-
- Vardo JH, Thornburg LL, Glantz JC. Maternal and neonatal morbidity among nulliparous women undergoing elective induction of labor. J Reprod Med 2011; 56: 25–30. - PubMed
-
- Dunne C, Da Silva O, Schmidt G, Natale R Outcomes of elective labour induction and elective caesarean section in low-risk pregnancies between 37 and 41 weeks’ gestation. J Obstet Gynaecol Can 2009; 31: 1124–30. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical