

Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response
- PMID: 30089911
- PMCID: PMC6095740
- DOI: 10.1038/s41586-018-0392-8
Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response
Abstract
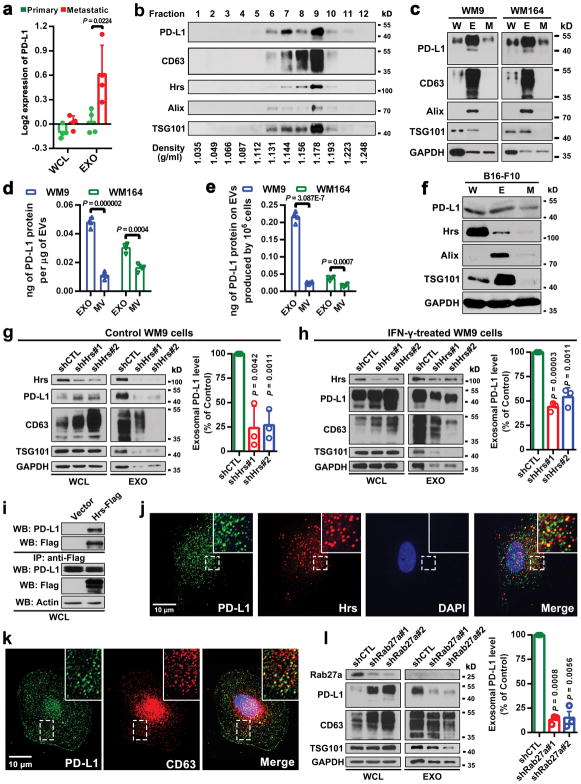
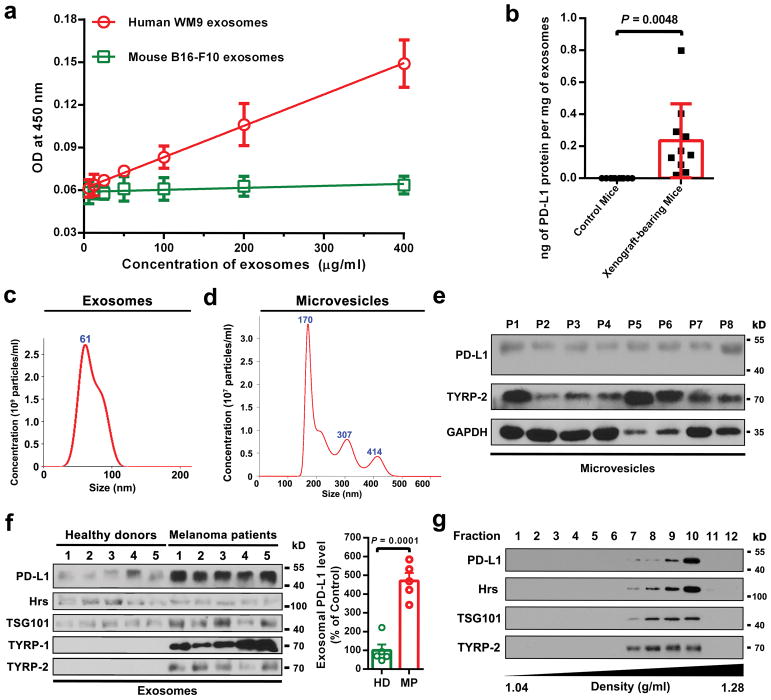
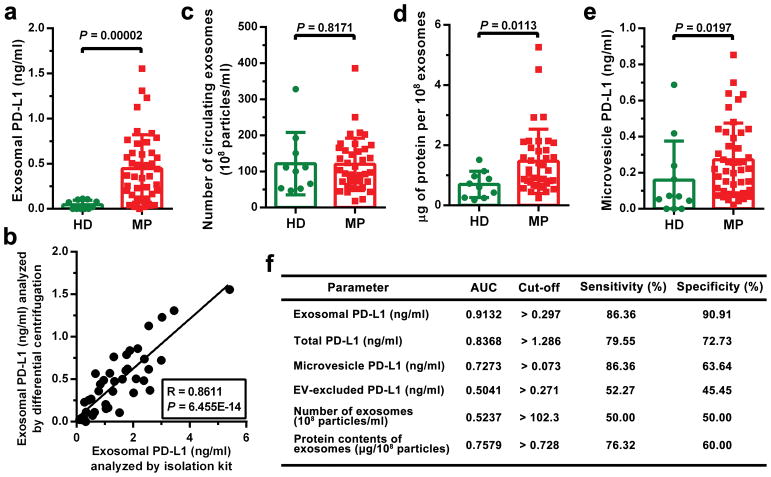
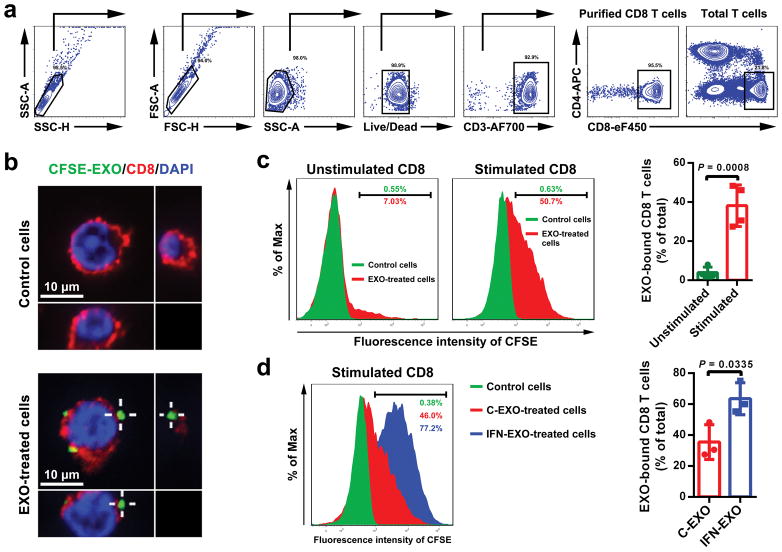
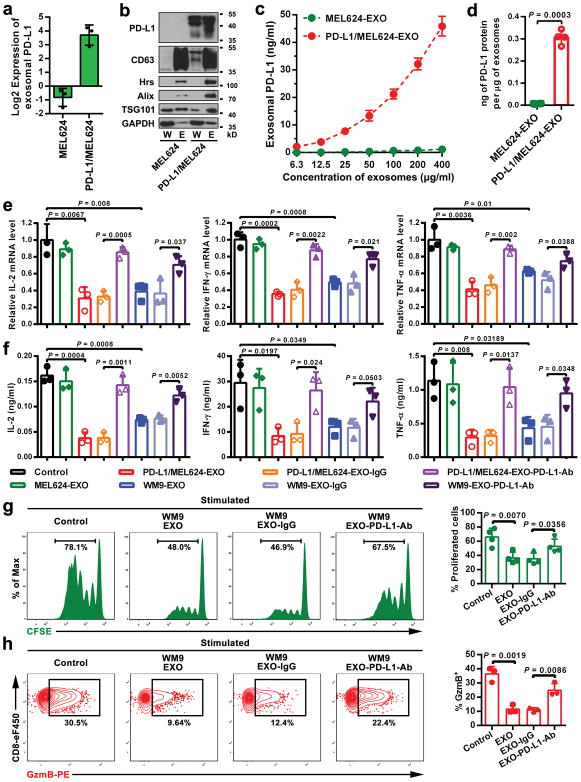
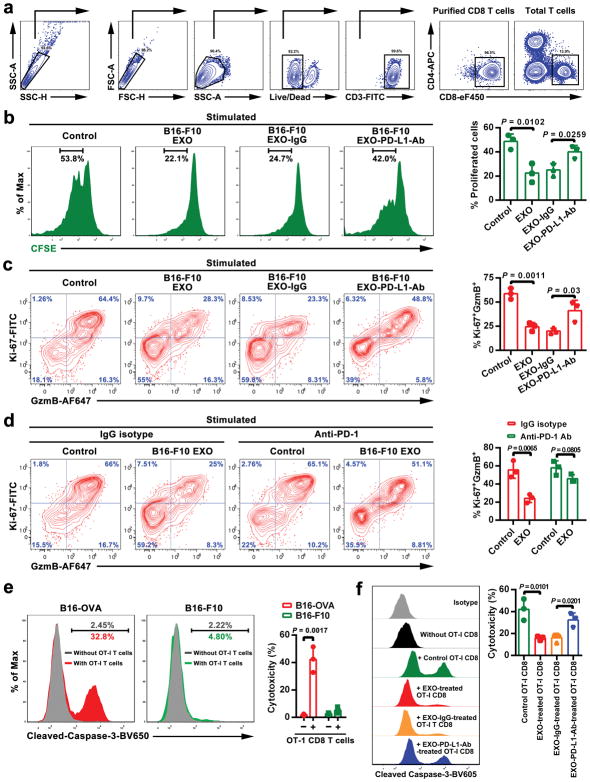
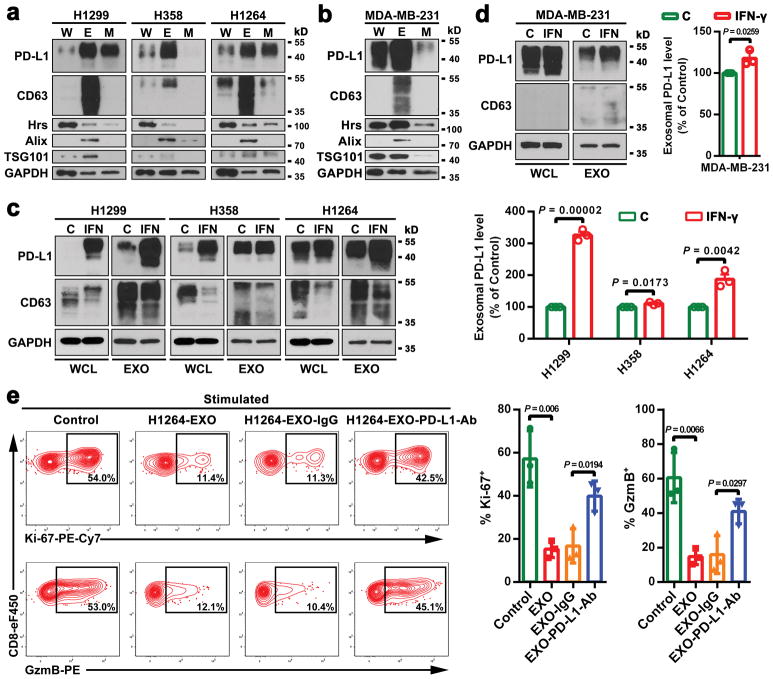
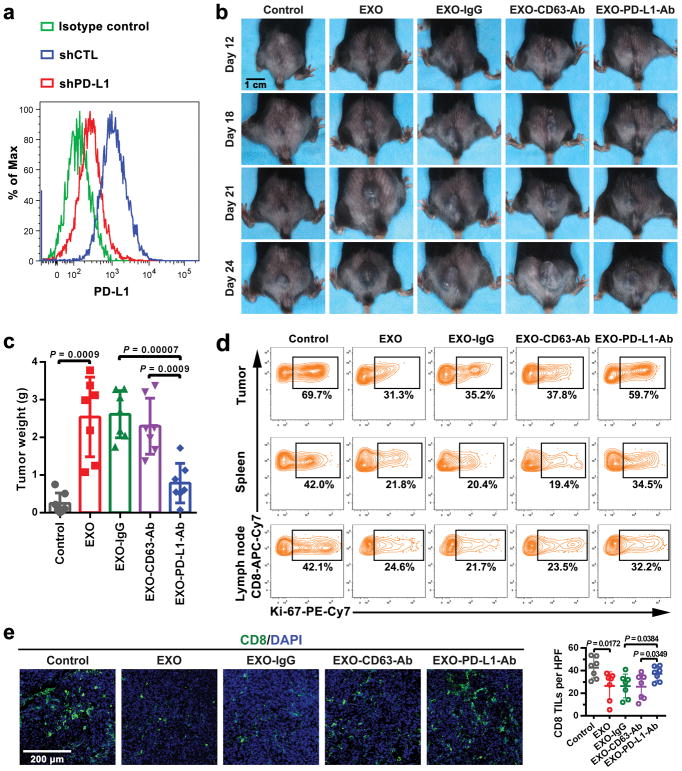
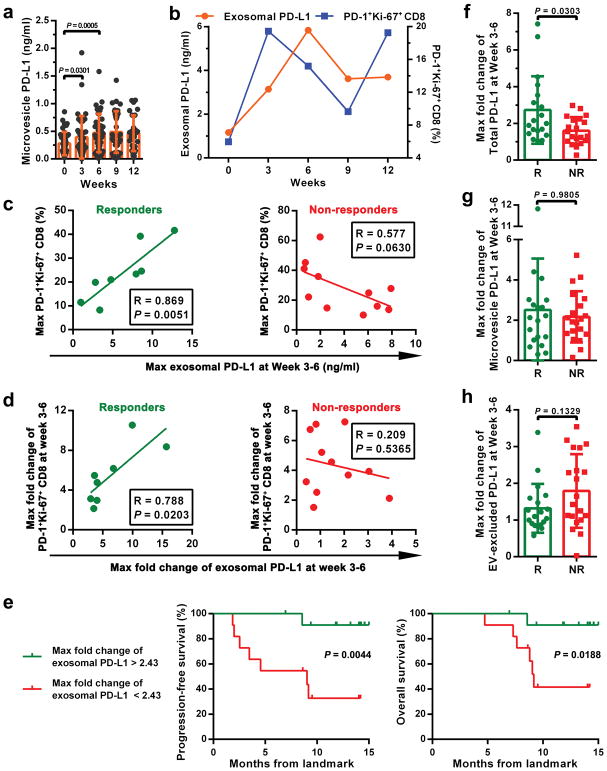
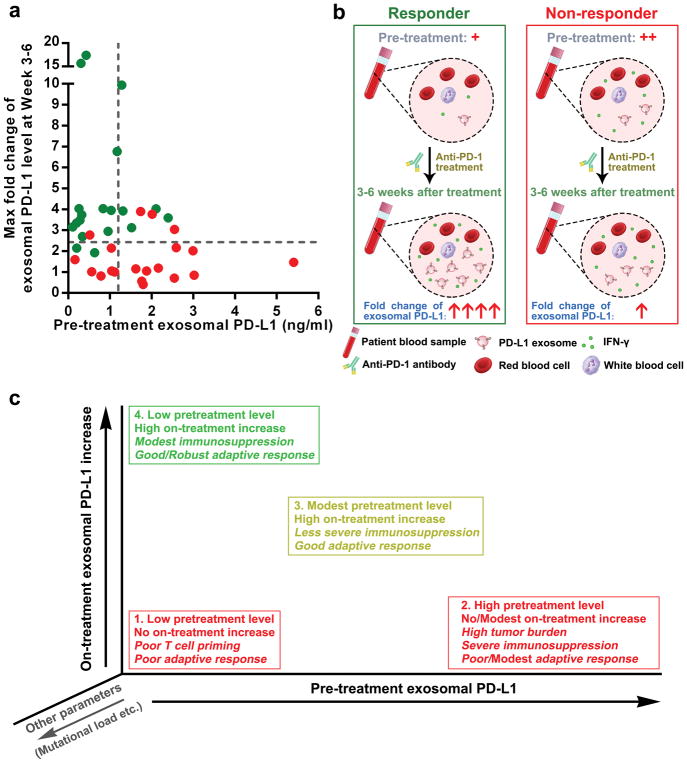
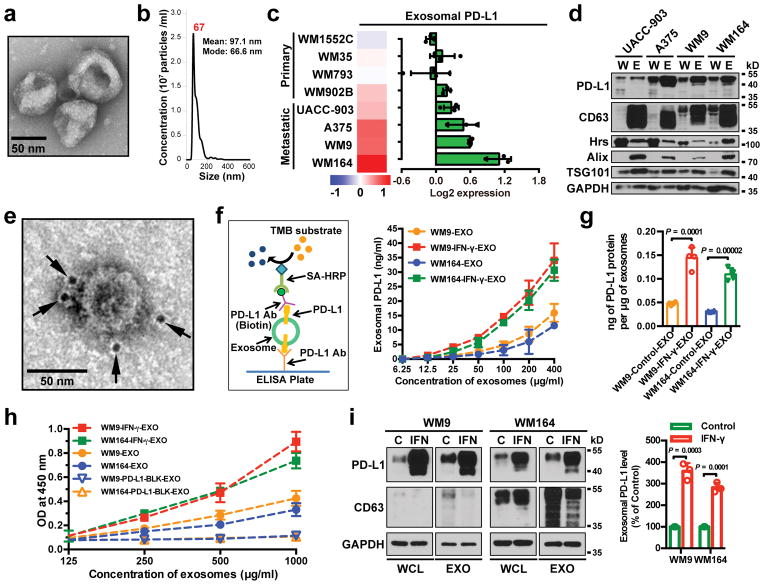
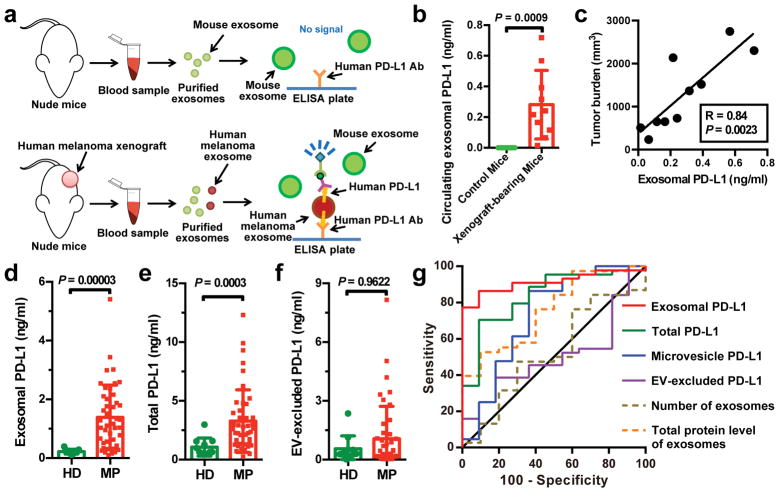
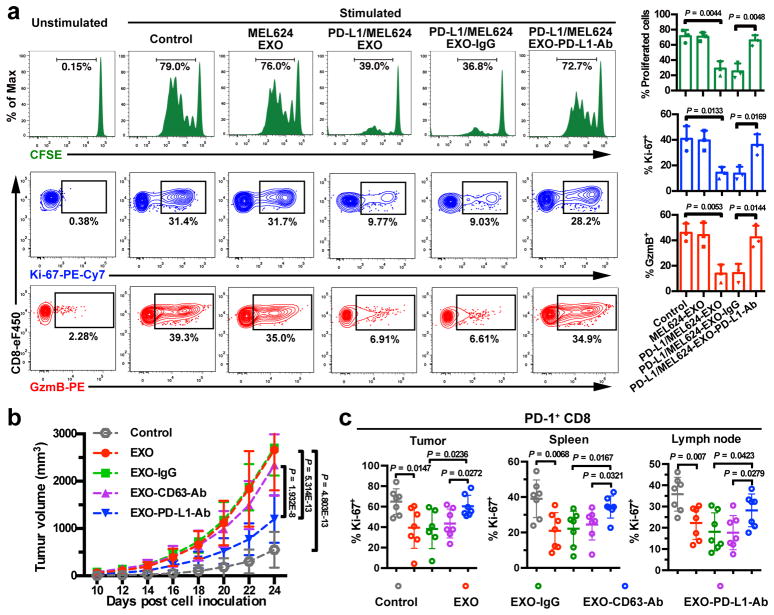
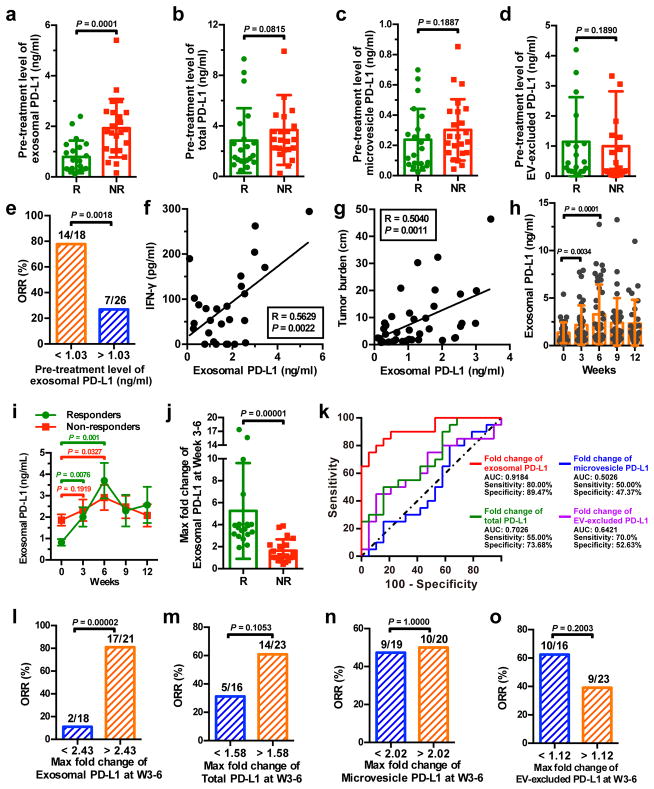
Tumour cells evade immune surveillance by upregulating the surface expression of programmed death-ligand 1 (PD-L1), which interacts with programmed death-1 (PD-1) receptor on T cells to elicit the immune checkpoint response1,2. Anti-PD-1 antibodies have shown remarkable promise in treating tumours, including metastatic melanoma2-4. However, the patient response rate is low4,5. A better understanding of PD-L1-mediated immune evasion is needed to predict patient response and improve treatment efficacy. Here we report that metastatic melanomas release extracellular vesicles, mostly in the form of exosomes, that carry PD-L1 on their surface. Stimulation with interferon-γ (IFN-γ) increases the amount of PD-L1 on these vesicles, which suppresses the function of CD8 T cells and facilitates tumour growth. In patients with metastatic melanoma, the level of circulating exosomal PD-L1 positively correlates with that of IFN-γ, and varies during the course of anti-PD-1 therapy. The magnitudes of the increase in circulating exosomal PD-L1 during early stages of treatment, as an indicator of the adaptive response of the tumour cells to T cell reinvigoration, stratifies clinical responders from non-responders. Our study unveils a mechanism by which tumour cells systemically suppress the immune system, and provides a rationale for the application of exosomal PD-L1 as a predictor for anti-PD-1 therapy.
Conflict of interest statement
W.G., C.G., and X. Xu. are listed as inventors on a patent owned by the University of Pennsylvania related to this work. W.G. and X. Xu. serve on the Scientific Advisory Board and have equities in Exo Bio, a company that has licensed the patent from the University of Pennsylvania.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 GM111128/GM/NIGMS NIH HHS/United States
- P01 CA025874/CA/NCI NIH HHS/United States
- P01 CA114046/CA/NCI NIH HHS/United States
- U54 CA193417/CA/NCI NIH HHS/United States
- U19 AI082630/AI/NIAID NIH HHS/United States
- P50 CA174523/CA/NCI NIH HHS/United States
- R01 GM085146/GM/NIGMS NIH HHS/United States
- R01 AI105343/AI/NIAID NIH HHS/United States
- R01 CA047159/CA/NCI NIH HHS/United States
- P30 CA010815/CA/NCI NIH HHS/United States
- U19 AI117950/AI/NIAID NIH HHS/United States
- T32 CA009615/CA/NCI NIH HHS/United States
- P01 AI108545/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
