Preoperative Electrophysiological Characterization of Patients with Primary Macula-involving Rhegmatogenous Retinal Detachment
- PMID: 30090179
- PMCID: PMC6058558
- DOI: 10.4103/jovr.jovr_161_17
Preoperative Electrophysiological Characterization of Patients with Primary Macula-involving Rhegmatogenous Retinal Detachment
Abstract
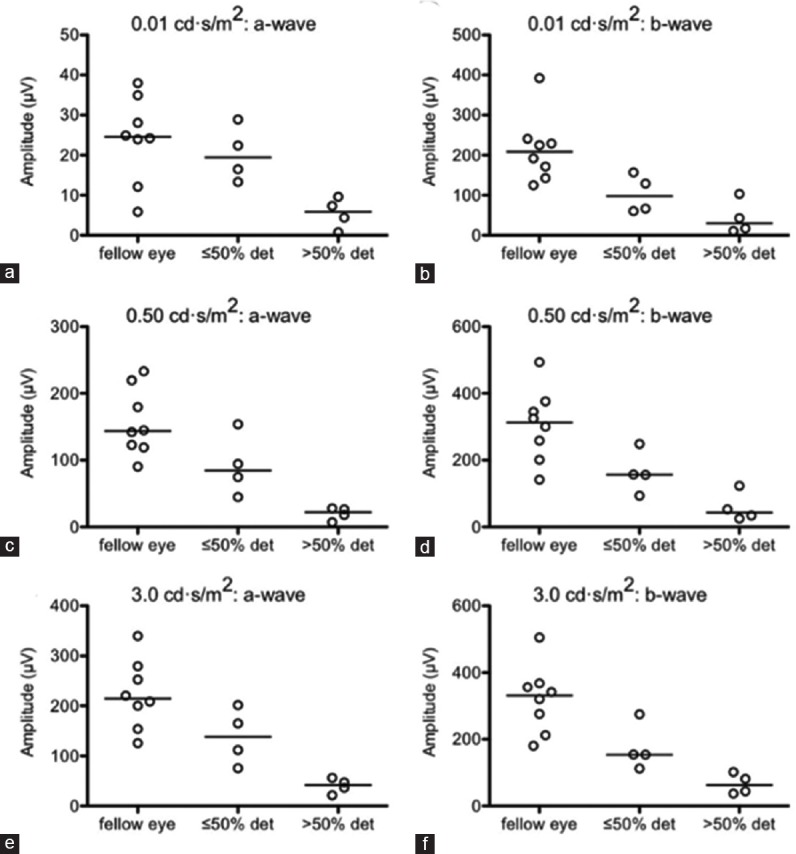
Purpose: To determine 1) which components of retinal function are impaired after rhegmatogenous retinal detachment, 2) which outer retinal pathways (rod- or cone-driven) are more severely affected, and 3) whether there is concomitant inner retinal dysfunction.
Methods: We conducted a prospective observational study in a large academic institution. We performed preoperative electroretinography on eight patients to assess outer and inner retinal function. In all cases, a comparison between the eye with the detached retina and the control fellow eye was made.
Results: Eyes with a detached retina had significantly lower a-wave and b-wave amplitudes with respect to both rod- and cone-dominated testing parameters (P < 0.05) and reduced 30 Hz flicker responses compared to fellow eyes (P < 0.05); the effect size was similar for all significantly reduced parameters (r~0.6). There were no significant differences between eyes with detached retinas and control fellow eyes with respect to b/a-wave ratios, a-wave latencies, or b-wave latencies.
Conclusion: Patients with rhegmatogenous retinal detachment have preoperative outer retinal dysfunction equally affecting both rod- and cone-driven pathways, and they have minimal inner retinal dysfunction.
Keywords: Clinical Electrophysiology; Electroretinography; Retinal Detachment.
Conflict of interest statement
There are no conflicts of interest.
Figures





References
-
- D'Amico DJ. Clinical practice. Primary retinal detachment. N Engl J Med. 2008;359:2346–2354. - PubMed
-
- Halberstadt M, Chatterjee-Sanz N, Brandenberg L, Koerner-Stiefbold U, Koerner F, Garweg JG. Primary retinal reattachment surgery: Anatomical and functional outcome in phakic and pseudophakic eyes. Eye (Lond) 2005;19:891–898. - PubMed
-
- Salicone A, Smiddy WE, Venkatraman A, Feuer W. Visual recovery after scleral buckling procedure for retinal detachment. Ophthalmology. 2006;113:1734–1742. - PubMed
-
- Mendrinos E, Dang-Burgener NP, Stangos AN, Sommerhalder J, Pournaras CJ. Primary vitrectomy without scleral buckling for pseudophakic rhegmatogenous retinal detachment. Am J Ophthalmol. 2008;145:1063–1070. - PubMed
-
- Kulkarni KM, Roth DB, Prenner JL. Current visual and anatomic outcomes of pneumatic retinopexy. Retina. 2007;27:1065–1070. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources