

Facet joint syndrome: from diagnosis to interventional management
- PMID: 30090998
- PMCID: PMC6206372
- DOI: 10.1007/s13244-018-0638-x
Facet joint syndrome: from diagnosis to interventional management
Abstract
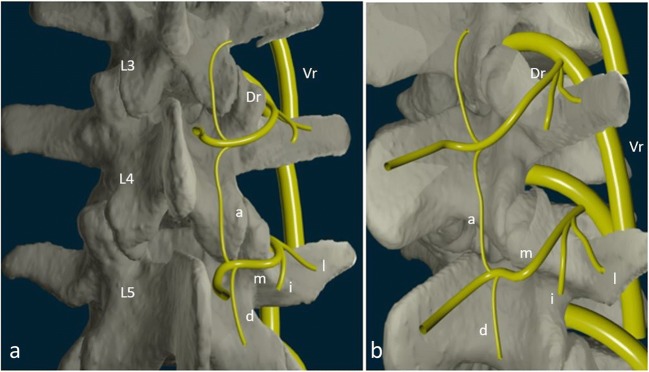
Low back pain (LBP) is the most common pain syndrome, and is an enormous burden and cost generator for society. Lumbar facet joints (FJ) constitute a common source of pain, accounting for 15-45% of LBP. Facet joint degenerative osteoarthritis is the most frequent form of facet joint pain. History and physical examination may suggest but not confirm facet joint syndrome. Although imaging (radiographs, MRI, CT, SPECT) for back pain syndrome is very commonly performed, there are no effective correlations between clinical symptoms and degenerative spinal changes. Diagnostic positive facet joint block can indicate facet joints as the source of chronic spinal pain. These patients may benefit from specific interventions to eliminate facet joint pain such as neurolysis, by radiofrequency or cryoablation. The purpose of this review is to describe the anatomy, epidemiology, clinical presentation, and radiologic findings of facet joint syndrome. Specific interventional facet joint management will also be described in detail. TEACHING POINTS: • Lumbar facet joints constitute a common source of pain accounting of 15-45%. • Facet arthrosis is the most frequent form of facet pathology. • There are no effective correlations between clinical symptoms, physical examination and degenerative spinal changes. • Diagnostic positive facet joint block can indicate facet joints as the source of pain. • After selection processing, patients may benefit from facet joint neurolysis, notably by radiofrequency or cryoablation.
Keywords: Block; Cryoablation; Facet joint; Low back pain; Neurolysis; Radiofrequency.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. - PubMed
-
- Manchikanti L, Singh V, Pampati V, et al. Evaluation of the relative contributions of various structures in chronic low back pain. Pain Physician. 2001;4(4):308–316. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
