

Sonographically indeterminate scrotal masses: how MRI helps in characterization
- PMID: 30091713
- PMCID: PMC6045519
- DOI: 10.5152/dir.2018.17400
Sonographically indeterminate scrotal masses: how MRI helps in characterization
Abstract
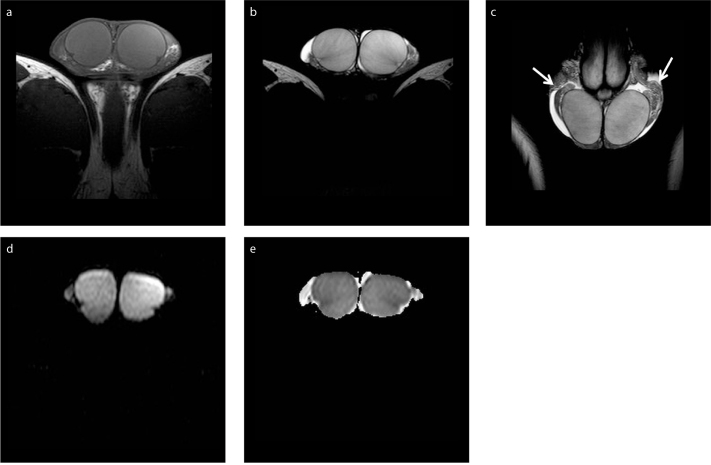
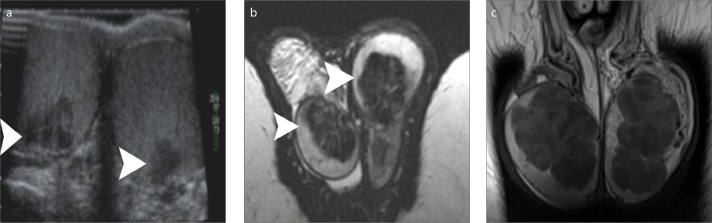
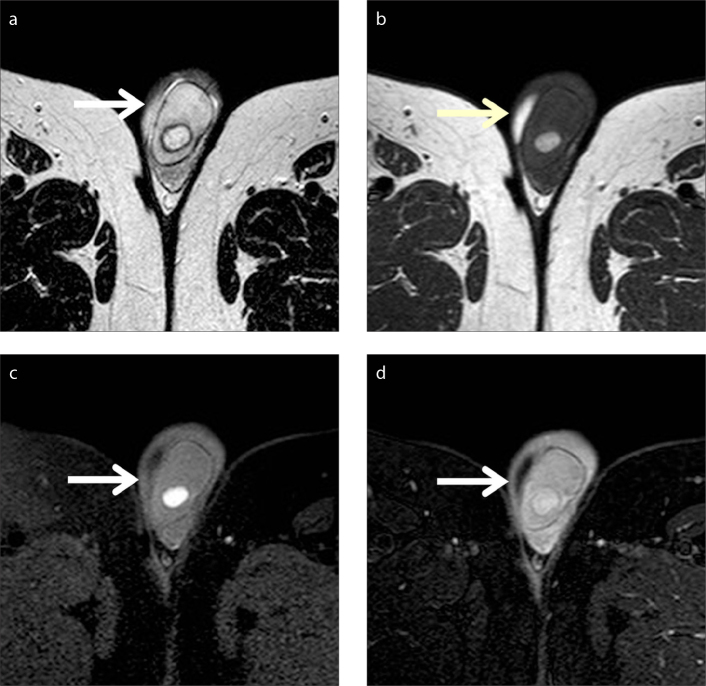
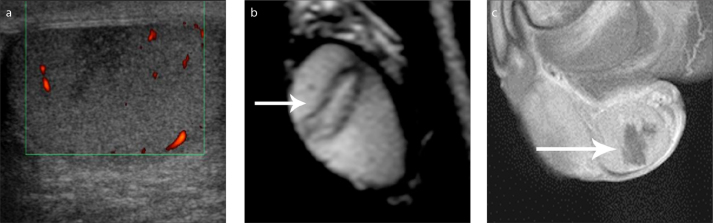
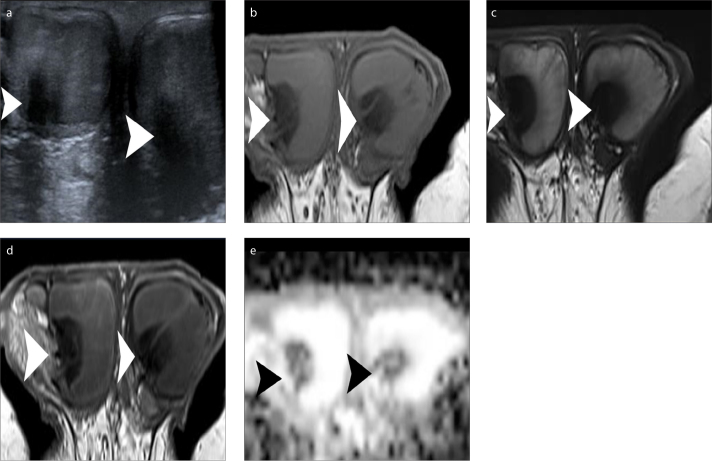
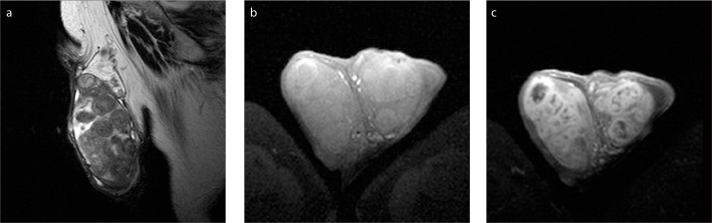
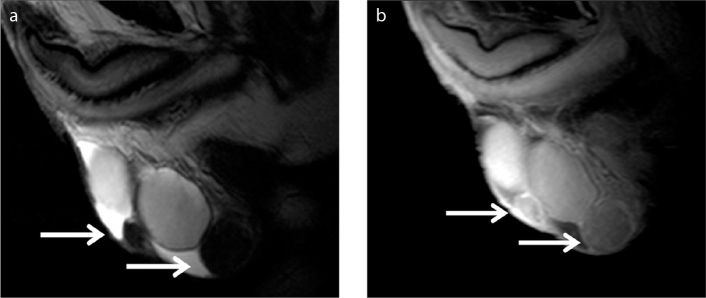
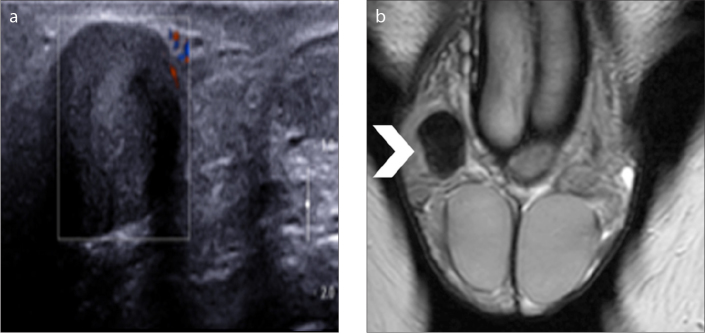
Magnetic resonance imaging (MRI) of the scrotum represents a useful supplemental imaging technique in the characterization of scrotal masses, particularly recommended in cases of nondiagnostic ultrasonographic findings. An accurate characterization of the benign nature of scrotal masses, including both intratesticular and paratesticular ones may improve patient management and decrease the number of unnecessary radical surgical procedures. Alternative treatment strategies, including follow-up, lesion biopsy, tumor enucleation, or organ sparing surgery may be recommended. The aim of this pictorial review is to present how MRI helps in the characterization of sonographically indeterminate scrotal masses and to emphasize the key MRI features of benign scrotal masses.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
